在中国,据统计2014年7 到 18岁的人群中近视发病率高达 57.1% [1]。 今年新冠导致大量儿童蜗居在家,网课成为学习的主要手段。恐怕接下来会迎来一波新的近视高峰。为什么近视这么普遍?有什么办法可以纠正或者控制近视的发展?
什么是近视?
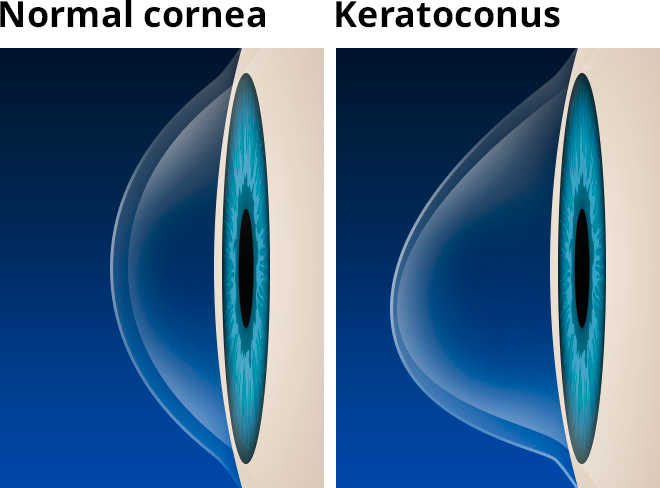
眼睛像个照相机,眼睛的整个透明介质包括角膜、晶体、玻璃体加在一起相当于镜头,视网膜相当于底片。光线被眼睛的透明介质汇聚后落在视网膜上我们就看到了清晰的图像(图一A)。近视的眼睛眼轴过长,导致远处来的光线不能到达视网膜(图一B),因此模糊。矫正近视可以在眼睛前面放个凹透镜,这样使得光线重新聚集在视网膜上。无论是镜框镜片,还是隐形眼镜片,或者之前讲过的角膜激光屈光手术,都是用这个原理矫正近视。这些方法,严格的来讲,只是治疗(treat),但不是治愈(cure)近视,因为眼轴的长度并没有变短。高度近视(大于等于600度近视)的一个后患就是由于眼轴增长导致视网膜脱离的风险增加。因此做了激光近视手术以后,虽然不戴眼镜看得也很清楚,但是视网膜脱离的风险并没有丝毫减少。顺便说一下,低度近视指300度以下,中度近视为300到600度之间。低度和中度近视的人视网膜脱离的风险大于正视(既不近视也不远视)的人,但是低于高度近视患者。

图一:近视的原理
假性近视vs真性近视
经常会看到各种文章提到假性近视,还有什么假性近视会发展成真性近视的说法。真性近视当然就是眼轴变长造成的近视。那什么是假性近视(pseudomyopia)?在这种情况,眼轴长度正常,但是眼睛汇聚光线的能力过强,因此光线还是聚在视网膜前方。眼睛里面有一块小小的环状肌肉叫做睫状肌(图一A),它的功能是调节晶体(图一A)的曲率。正常人的眼睛看远处时,睫状肌放松,晶体扁平;当看近处的时候,睫状肌收缩,晶体变凸,眼睛汇聚光线的能力变强。这样不论看远还是看近光线都可以汇聚在视网膜上。看近处时睫状肌收缩导致晶体汇聚力加强这一过程叫做调节。和身体别处的肌肉一样,睫状肌也会疲劳,有时也会痉挛。如果一直处于收缩状态,眼睛的汇聚光线力过大,远处的光线就会聚在视网膜之前,造成和近视一样的看远处模糊。
这种假性近视本质上说是眼睛调节能力的失调的一种。青少年学习时间长,加上眼睛还处于发育过程,调节能力失调时有发生。因此儿童和年轻人配眼镜,标准的方法是要用散瞳眼药水将睫状肌麻痹,迫使它放松,然后再验光,否则不能准确。我在临床上看过太多例子,自然状态下有低度近视(100度左右),散瞳后是平光甚至远视。甚至有一个已经33岁的西裔女子,多年来验光度数起起伏伏,大约近视100到200度,我给她散瞳后发现她其实有100度的远视,解释了她没法容忍近视眼镜,而且平时看书会累的症状。我还见过一个极端例子,13岁男孩从未戴过眼镜,自动验光仪测出900度近视,自述看东西模糊,视力表只能看清最上边0.05的字母。后来在验光的过程中,他的调节痉挛逐渐缓解,最终裸眼看到了1.0。显然这个小朋友没有近视,他需要的是视觉训练来帮助他恢复眼睛正确的调节功能。
以前人们以为真性近视是由假性近视发展来的。现在知道,这两者没有什么必然的关系。近视是眼轴过长,而假性近视作为眼睛功能失调的一种,不能算是严格意义上的近视。
那么为什么眼轴会增长?
眼睛的生长是由视网膜局部的信号来调节的。当眼睛清楚得看到一个物体时(也就是光线聚焦在视网膜上的时候),眼睛得到的信号是:一切正常,不需要生长。当长期注视近距离的物体时,光线会稍微聚焦在视网膜后边一点的位置上,视网膜得到的信号是:现在清晰度不是最优,我要稍微往后靠一点才能逮住这些光线。这样眼睛就稍微长长一点,长此以往近视就会不断加深。而且眼睛收到信号之后要么不变,要么生长,没有逆生长,换句话说,眼轴要么不变,要么变长。
人类的眼睛本来就不是设计来看近处的。远古的人类需要好的远处视力以便能够找到哪棵树上有果子,哪里有只兔子可以去捉住,或者那地平线上是不是有只狮子跑过来了。远古人类的平均寿命假如按照40岁算的话,还没来得及老花眼就死了,所以看近处从来不是问题。更何况,基因早在生育年龄就流传下去了,所以老花眼在进化中没办法被淘汰。总之,人的眼睛生来就是用来看远的。需要看近处的时候,动用一下眼睛的调节力,也就是睫状肌发力让晶体变凸从而让光线继续聚在视网膜上。不过,人的眼睛倾向于不过分工作,也就是有个轻微的小折扣,实际上光线没有正好在视网膜上,而是在视网膜后边一点点。问题就在于偶尔这么干还行,一天10小时看着书或者手机,这种信号就是让眼轴长长长。
近视有什么危害?
- 不能当飞行员
- 找不到男/女朋友
抛开玩笑,很多人觉得近视没什么大不了的,无非就是戴眼镜不太方便,况且现在还有各种隐形眼镜和激光手术。但是近视,尤其是高度近视(大于600度),由于眼轴的增长,会增加各种眼睛疾病的风险,包括视网膜脱离,巩膜新生血管,白内障,青光眼和黄斑萎缩 [2],这些疾病可以造成永久性失明。由于近视的发病率非常高,而1/5的近视是高度近视,算下来非常可观的人数有着这些永久失明的风险。而戴眼镜和激光手术并不能降低这些风险,原因是眼轴长度并未得到改变。
哪些因素会影响近视的发展?
近视是由基因和环境相互作用造成的。近视发展的风险因子包括:
- 家族历史。父母双方都近视的孩子的近视风险是父母双方都不近视的孩子的2倍还多。这个很好理解,基因的作用不容忽视。另外还有一些环境因素,比如近视的父母一般看书时间长,孩子也容易更喜欢看书。
- 近距离用眼的时间。工作性质、教育程度等等,这些不言而喻。
- 6-9岁时的眼睛屈光度。乍一看这点很奇怪。事实是,婴儿刚刚出生时的眼睛平均屈光度为200度远视(有很广的范围,从600度近视到1100度远视,但是大部分新生儿集中在200度远视左右),注意是远视而不是近视。然后在18个月的时候这种人与人之间巨大的区别就基本消失了,大家都差不多稳定在125度远视,这一过程叫做正视化(Emmetropization)。正视化是指眼睛生长发育达到正视,眼睛的聚光能力和眼轴的长度吻合的状态。可以想象,如果按照古代狩猎和畜牧的生活方式,人眼睛的这个度数就定了,直到病死饿死或者被老虎吃了。我们无从考查古代人的眼睛度数,但是一个非常有趣的例子是巴西亚马逊热带雨林的一个部落,至今没有太多的被现代文明侵入。我的一位老师,在近视研究领域内的一位先驱,曾经去那个村子考察当地居民的眼睛屈光度。在这个几百人的村子里,平均屈光度为75度远视,只有4个人有大于100度的近视。这四个人中,两个是村子里唯二的大学生,职业为老师,经常阅读;一个从儿童时代起就做裁缝;还有一个是个出生就高度近视的先天盲人。
由此可见,我们绝大多数人生来都不是近视眼,不幸的是,文字出现,书籍出现,ipad出现。现代人类的近视大概从7-9岁开始,每年增长100度;或者如果从10-13岁开始,则每年增长较慢,大约50度。近视的增长一般在17-23岁停止,但是像我之前在近视激光手术文章里讲的,成年人也可能会有缓慢的近视发展 — 多谢现代人的生活方式。
统计发现,6岁时候的眼睛屈光度如果是75度远视,那么将来近视的风险大为降低;相反,如果低于75度远视的话,则近视风险升高 [3]。
- 种族: 近视青睐系数亚裔大于白人大于黑人 [4]。具体和基因还是文化、环境的差异有关,不得而知,可能都有关系。
- 户外活动时间。最新的研究表明,户外活动,不管是运动还是静坐,不管是远眺还是读书,都会减少近视发展的几率和程度[5 , 6]。具体的机制是什么?加强了昼夜节律,更多的眺望了远处,在户外阳光下通过小瞳孔视力更加清晰,紫外线的照射,强烈的户外自然光促使视网膜合成多巴胺?还是由于维生素D的合成?现在还不清楚,也许是多种原因吧。
- 规律的昼夜节律对眼睛的正常发育和正视化是必要的。婴儿期和儿童期晚上睡觉开夜灯会增大日后近视的风险。研究表明两岁前在黑暗中睡觉的婴儿后来只有10%的近视;那些开着夜灯睡觉的孩子后来有34%的近视;而那些开着正常灯睡觉的小孩后来的近视率有55% [7, 8]。
参考文献
2. Wu, P.C., et al., Epidemiology of Myopia. Asia Pac J Ophthalmol (Phila), 2016. 5(6): p. 386-393.
7. Quinn, G.E., et al., Myopia and ambient lighting at night. Nature, 1999. 399(6732): p. 113-4.