This article is for eye doctors who use axial length routinely in their myopia control clinic, and certain parents who are curious and/or obsessed with the numbers of their children’s eyes (trust me, I do encounter these parents weekly).
Briefly, axial length is the length of the eyeball, which grows throughout the first 18 years of a person’s life. It is normal for the eyes to grow longer over time until it stabilizes at adulthood. But the growth can be accelerated resulting in long axial length in myopia. Therefore in many eye doctors’ offices, this value is measured to monitor myopia development and record whether myopia control is successful with a given intervention.
Understandably, it is important to have a normative database to evaluate whether a given child’s axial length is normal. Basically, there have been quite a few published articles on typical axial lengths of children of various ages. I have put together data from two recent studies that encompass ages from 3 months to 18 years below. The mean values for a given age are listed, as well as standard deviation. Table 1 is from Florida, USA, on 165 American children (Miami study) [1] and table 2 is from Shanghai, China, on 14,127 Chinese children (Shanghai study) [2]. Obviously the 2nd study is a much larger scale, and I really am very excited about this very new data. The first study, though with much fewer subjects, is quite remarkable as well in my opinion, as it examined kids as early as 3 months, understandably not easy to do and not many other studies were able to look at this age group. So I am keeping these two tables as a reference for my own patients.
For those who are more visual, Figure 1 and Figure 2 are these numbers plotted in graphs.
Table 1. Axial length of 3 month to 7 years old children (Miami study)
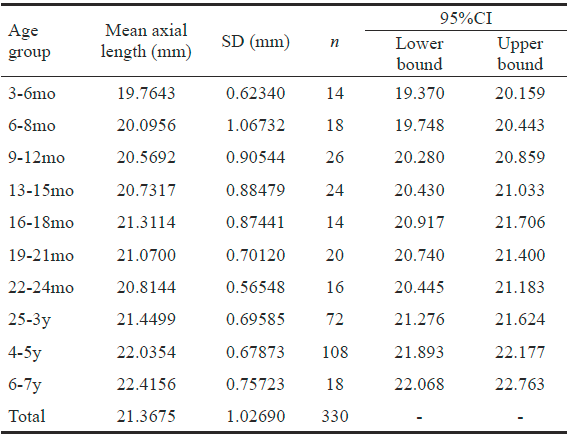
Table 2. Axial length of 4 to 18 years old children (Shanghai study)


Figure 1. Axial length mean (solid line) and 95% confidence interval (dotted lines) in 3 month to 7 years old children (Miami study).
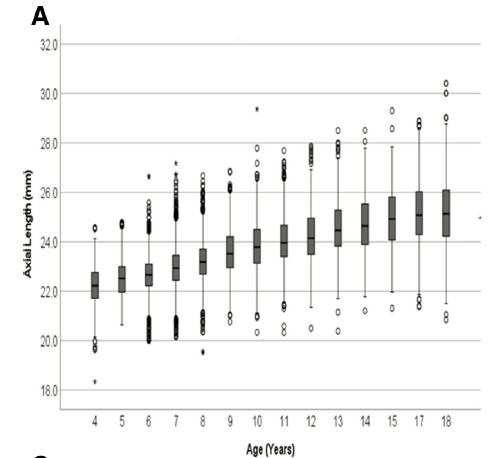
Figure 2. Axial length ranges in 4 to 18 years old children (Shanghai study).
A few things to keep in mind from these data.
First, these are from two distinct populations. The 3 month to 7 years old study group (Miami study) were children from Miami, FL. No ethnic background information was given in the paper, but one can assume it could be typical from that area. The 4 to 18 years old study group (2nd Shanghai study) were Chinese children. It is well known that Chinese children have longer axial lengths than Caucasions and African descents (and more prevalent myopia rates unfortunately), so we certainly cannot assume that this is inclusive of all possible scenarios.
Second, you can see that for any given age, there is a wide range of axial lengths in both studies. This tells us that normal is a range, NOT a single number. Do NOT compare the number of your child to your neighbor’s kids. This is not a competition. Also, it has been demonstrated again and again that it is the rate of axial length growth, rather than the absolute number, that better predicts myopia progression. Do not get anxious over one measurement. Monitor the axial length over time to find the trend.
Lastly, I would still stress that while it is great that we have a normative database for axial length, it is still the gold standard to perform cycloplegic refraction to accurately assess a child’s true refractive error. Axial length measurement is a powerful tool, but it does not and cannot replace cycloplegic refraction.
References:
[1] Miami study: Bach A, Villegas VM, Gold AS, Shi W, Murray TG. Axial length development in children. Int J Ophthalmol. 2019;12(5):815-819. Published 2019 May 18. doi:10.18240/ijo.2019.05.18
[2] Shanghai study: He X, Sankaridurg P, Naduvilath T, Wang J, Xiong S, Weng R, Du L, Chen J, Zou H, Xu X. Normative data and percentile curves for axial length and axial length/corneal curvature in Chinese children and adolescents aged 4-18 years. Br J Ophthalmol. 2021 Sep 16:bjophthalmol-2021-319431. doi: 10.1136/bjophthalmol-2021-319431. Epub ahead of print. PMID: 34531198.
