A case of recurrent corneal erosion
Transcript for those of you who would rather read:
A middle aged female patient came in, referred by one of the ophthalmologists in our practice for dry eye treatment. She said, ‘Oh I did not know that you were an optometrist, I thought you were a dry eye specialist.’ This statement assumes that an optometrist cannot be a dry eye specialist. That is plainly wrong. However, I can only imagine that she is not alone here and it may represent a popular misconception. Contrary to what the public think, an optometrist does not only prescribe glasses or contact lenses, though these are certainly the bread and butter in our jobs. An optometrist can diagnose and treat most eye diseases, and many of us develop specialties such as dry eye, medically necessary contact lenses, low vision, vision therapy and pediatrics. For dry eye, there are probably more specialists that are optometrists than ophthalmologists. I may do another video in future about how to select the right eye doctor based on your needs and visual complaints.
I said, ‘dry eye is a specialty that both optometrists and ophthalmologists can do. Tell me your problem and I’ll see if I can help you.’
Though she did have chronic dry eye in both eyes, it’s her left eye that she was mostly worried about. (You can learn more about dry eye in my previous video and blogs and I have linked them below in the video description. )
She initially had an injury of the left cornea 8 months ago because of using CPAP mask while sleeping, since then it had happened again and again, to the point she had to discontinue using CPAP. The cornea is the clear tissue on the surface of the eye and good vision relies on clear and healthy corneas. Dry eye and injury can both make this tissue sick and result in pain, tearing and poor vision.
Her first ophthalmologist performed a procedure to remove the faulty superficial layer of the cornea and put a bandage contact lens in to protect the eye. Unfortunately that resulted in a corneal ulcer, for which she had to go to the emergency room of a famous eye hospital in a different city. A corneal ulcer is an infection of the cornea, which can lead to permanent vision loss if untreated. One of the risk factors of developing corneal ulcer is wearing contact lenses, and some of the contact lens related corneal ulcers can be difficult to treat, especially with delayed treatment.
With intensive antibiotic eye drop treatment, the corneal ulcer resolved. But her nightmare of the cornea injury continued, she was having almost weekly recurrent corneal erosions in the left eye, waking up with eye pain. She could not sleep well and was afraid to open her eyes in the morning.
So what is recurrent corneal erosion, or RCE? This is typically a tear of the superficial layer of the cornea, initially often from an injury, but subsequently can happen spontaneously. It often happens when people wake up in the morning, because a sudden opening movement of the eyelid can open up a previously weak spot in the cornea. In addition, many people have dry eyes overnight for various reasons, such as incomplete closure of eyelids, having heat or air conditioner on, using a cpap machine, etc. Having dry eyes predisposes the opening of the healed wound again. As a result, waking up with severe pain, tearing and light sensitivity in the eye is a common complaint for those with RCEs.
How do you treat RCEs? First, it is imperative to keep dry eye under control, for the reason mentioned above. This is also the reason my patient’s ophthalmologist referred her for dry eye treatment. Second, special attention should be given to the enticing factor of the cornea wound. In her case, it would be the overnight incomplete eyelid closure and possibly the eye touching pillow or other things physically.
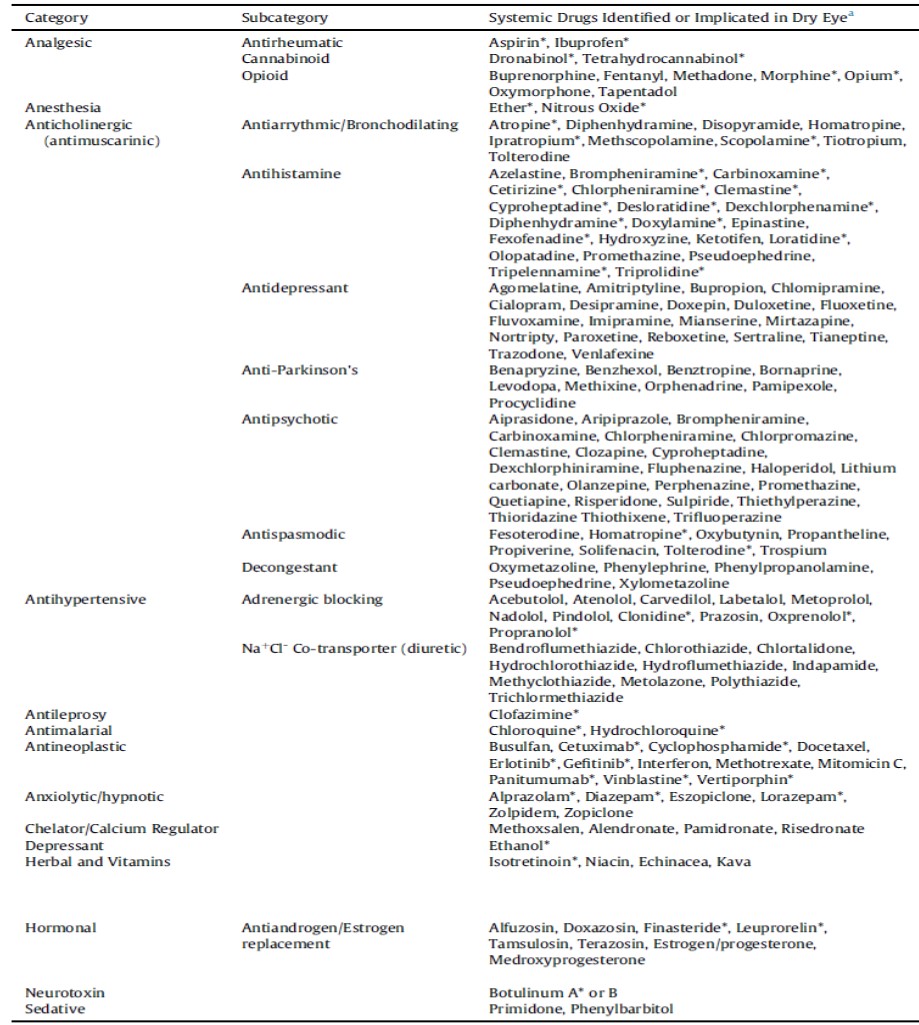
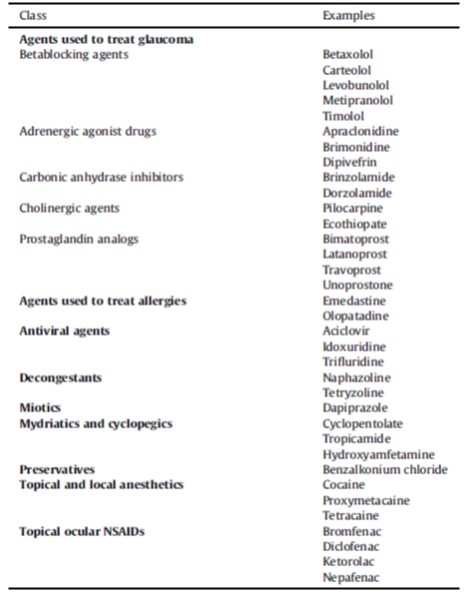
She had already tried ointment at night which did not prevent RCE from happening. She used artificial tears during the day, but the relief was only temporary. She was not doing any warm compress because she needed to boil her eye mask for some minutes to reactivate it each time. She did take fish oil capsules. The fish oil and the stopping of her amitriptyline medication were the only things that seemed to be helpful to her. Yes, certain medications can cause dry eye and again you can find more information in my link below. She was using steroid drops while her cornea was healing but she could not use that forever due to side effects such as cataract and glaucoma. She tried various goggles but reported that when they moved at night she sometimes found her eye touching various parts of the goggles, which could make things worse.
Careful examination of her eyes showed that she had meibomian gland dysfunction and ocular rosacea, which were contributing factors to dry eye. More information about these conditions can also be found in my previous blogs with the link below.
Based on her past treatment, I recommended that for dry eye and MGD, she continue the artificial tears 4 times a day, but should buy a much easier to use eye mask which can be simply heated up in the microwave before use. She would need to do warm compress twice with 5 min each time daily. She would continue the fish oil, which was beneficial to dry eye. She could start restasis twice daily, this being an FDA-approved eye drop for chronic dry eye, but with the caveat that it could take up to 3 months to be effective, and it only worked in a small percentage of dry eye patients. In future, if her dry eye is still not controlled well, she would benefit from intense pulsed light therapy, which is unfortunately very expensive and not covered by insurance.
For RCE, I recommended that she use a large amount of ointment in the left eye at night, and put an eye shield on to prevent things from getting onto or into the eye. Some studies suggest that doxycycline can prevent corneal breakdown and reduce the frequency of RCE. So I prescribed that to her. She did have stomach upset previously when taking it for Lyme’s disease, but this was a reduced dosage and we will monitor GI side effects closely.
Patient was very thankful and I hope she got better. Long-term management is required for both RCE and dry eye. That’s it for now. Let me know your thoughts and comments. See you next time!
Links for dry eye and MGD: https://bostoneyeblink.com/2016/06/28/why-are-your-eyes-dry/
When artificial tears just don’t cut it – Other treatments of dry eye
ocular rosacea: https://bostoneyeblink.com/2019/12/12/another-treatment-for-dry-eye-doxycycline/
systemic medications that are associated with dry eye: https://bostoneyeblink.com/2019/11/02/when-drugs-cause-dry-eye/