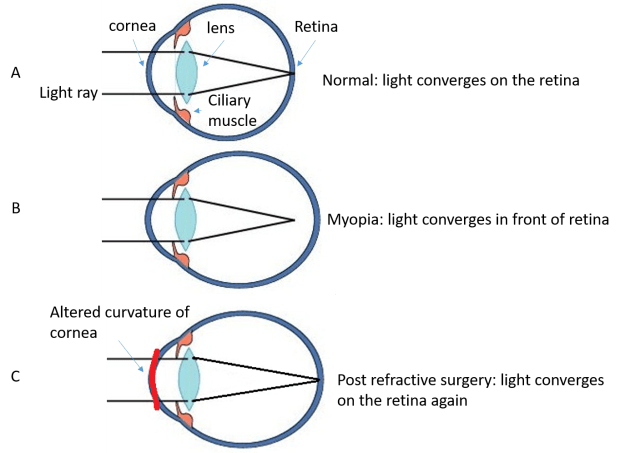
Phakic IOLs are small lenses implanted in the eye to correct refractive error. So far, FDA has approved two lenses to be used for correcting myopia up to -20.00 diopters (D) with astigmatism up to 2.50 D for people 21-45 years of age. These are alternatives to corneal refractive surgery such as LASIK, especially for high myopia, because too much corneal tissue needs to be removed in high myopia in LASIK and it becomes unsafe. As a comparison, LASIK is FDA approved for myopia up to -11.00 D. Click here to read my post on LASIK.
Two implantable lenses approved by FDA
- The Visian ICL (Implantable Collamer Lens), approved in 2005, is placed behind the iris and in front of the natural lens. It is invisible to the naked eye. The Visian ICL is made of a soft, biocompatible collagen copolymer, and can be folded during implantation, requiring only a small incision of 3 mm.
- The Verisyse (branded as Artisan in Europe), approved in 2004, is placed in front of the iris, also called an iris-claw lens. The Verisyse lens is made of a rigid plastic, and because it cannot be folded, it requires a larger incision of 6 mm. If you look very carefully, you may see the lens with naked eyes.
Are you a good candidate for pIOL implant?
As mentioned earlier, patients with high myopia outside the range for LASIK can have pIOL implant to correct myopia. However, you still need to meet certain requirements to be a good candidate. Below are some of the important factors to consider.
- pIOL is approved for myopia up to -20.00 D, not higher
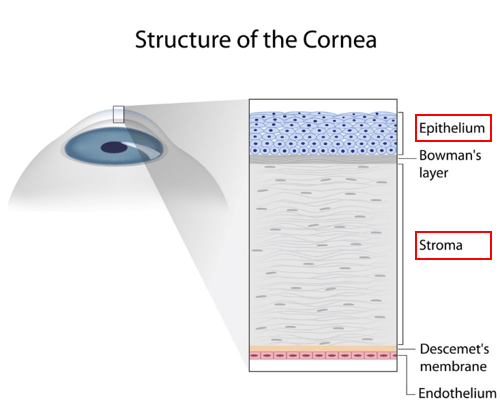
- Two important parameters of the eye need to be determined: the anterior chamber of your eye has to be deep enough; and your corneal endothelium needs to be healthy. This is because the implanted lens needs to have enough room in the eye, otherwise it may block the drainage system of the eye and causes increased eye pressure and glaucoma. In addition, the surgery itself and the lens often cause loss of corneal endothelial cells, as will be discussed further later, therefore a healthy corneal endothelium is also a pre-requisite.
- You must have had stable glass prescription for at least a year.
- Eye conditions such as cataracts, glaucoma and untreated eye infections will prevent you from being a good candidate.
- Systemic contraindications include Sjogren’s syndrome, rheumatoid arthritis, diabetes, HIV and AIDS, and certain medications such as steroids and immunosuppressants may interfere with healing and final outcomes.
What does the surgery involve?
Prior to the surgery, a procedure called laser peripheral iridotomy (LPI) will be performed on the eye that will receive the implant. This procedure makes a hole on the periphery of your iris to prevent the eye pressure from going up during and post-surgery. LPI can be done a week before or on the same day of the surgery. A newer model lens available in Europe and China but not in the US at the moment, Visian ICL V4c, which has a 0.36 mm diameter hole in the center of the lens, allows fluid exchange without the need of this extra procedure.
The surgery itself takes 10 to 30 minutes and is performed on an outpatient basis. Numbing eyes drops are applied, then small incisions made on the cornea to allow the lens to be inserted into the eye. Here is a demonstration video showing the procedure of Visian ICL: https://www.youtube.com/watch?v=wlaAYBefNTo; and for Verisyse lens: https://www.youtube.com/watch?v=Y4GUpMAHA9s.
After the surgery, you will be given antibiotic and anti-inflammatory eye drops to prevent infection and inflammation.
Most patients will notice clear vision shortly after the surgery and their vision stabilizes within a week, but for some patients it may take a few weeks. There is minimum pain although foreign body sensation can be common after the surgery. Most people can resume work and normal daily activities within a few days.
Safety and Efficacy of pIOLs
Phakic IOL implantation is considered to be safe. However, this is still an open-eye surgery, so risks including retinal detachment and endophthalmitis (infection of the entire eye) due to the surgery exist. Generally, the surgery risk is less than that of cataract surgery, but more than LASIK where the eye remains a closed system.
The two types of pIOLs showed equal and comparable safety, predictability, and efficacy [1].
The accuracy of the optics is decent. For Visian ICL, in 41 eyes of 41 patients with myopic refractive errors of -4.00 to -15.25 D, at 8 years, 68.3% and 85.4% of the eyes were within 0.5 and 1.0 D, respectively, of the targeted correction [2].
The vision post-surgery is also good. In FDA trials, the Verisyse have been shown to have 20/40 uncorrected visual acuity (UCVA) or better in 84% of patients after three years and Visian ICLs have been shown to have an UCVA of 20/40 or better in 81% of patients after 3 years [3]. A different study found 60.5% eyes with UCVA 20/20 or better [4].
Considering that this patient population typically have myopia -10.00 D and more, it is not hard to imagine that patient satisfaction is high overall.
So in summary, pIOLs to correct myopia show good safety and efficacy. It may not be completely fair to compare the UCVA post pICLs vs LASIK, as patients in pICLs typically are more myopic than those in LASIK, and we know that some high myopes may not achieve best corrected VA of 20/20 due to myopic retinal changes.
Just by looking at the numbers, the percentage of eyes within targeted correction appears to be lower than that of LASIK (98.6% of eyes reach refraction within 1.00 D of target, and 90.9% of eyes reach within 0.50 D of target refraction). Given that we are comparing two types of refractive surgeries in two different patient populations, one cannot make a conclusion that LASIK achieves better correction than ICL; but as a patient, you can roughly estimate your chance of getting the ideal correction if you are a candidate for LASIK or pIOL.
Complications of ICL
There are several complications, most common are cataract and corneal endothelial cell loss. Verisyse lenses and Visian ICLs are similar, since Visian ICLs are better studied, I will use ICLs as an example for this section. Below are data summarized by a recent meta-analysis [5] unless otherwise indicated.
ICL replacement
The surgery is reversible, meaning that the implant can be taken out or replaced if it is not ideal. Still, no one likes to have a second surgery. Fortunately, only 1.0-2.6% of cases require a replacement of ICL. The common causes for replacement include too long or too short of a distance between the implanted lens and the natural lens.
Cataract
ICL induces a specific cataract called anterior subcapsular cataract (ASC) due to close proximity of the implant to the front part of the natural lens. Based on 8 studies, it is estimated that the incidence of ASC due to ICL implant ranges from 1.1% to 5.9%, and the incidence of ASC cataracts requiring surgery ranges from 0% to 1.8%.
Another review looking at 2592 eyes showed ASC in 5.2% cases, of these, 43.4% were reported within 1 year, 15.4% between 1 and 3 years, and 35.3% ≥ 3 years after ICL implantation [6].
Even though the cataract incidence due to implants remains low, it has been found that for older patients (>40 years of age) and higher myopia (-12.00 D or higher), the risk of cataract were much increased, as high as 28% at 6 year follow up.
High myopia itself is a risk factor for ASC post ICL implant. While clinically significant cataracts occurred in seven (6.6%) of 106 eyes with preoperative myopia of −12.00 D or higher, none occurred in the 420 eyes with preoperative myopia lower than −12.00 D.
Corneal endothelial cell loss
Corneal endothelial cells are important in keeping the cornea clear. These cells do not regenerate and we lose about 0.4% of them every year as a result of normal aging [7]. ICL implantation accelerates the endothelial cell loss to about 7.5% loss at 5 year follow up. Fortunately, this stabilizes after 2-3 years.
Glaucoma
Lens implantation may cause release of pigment from the iris, blocking the drainage system of the eye, thereby increasing eye pressure, leading to glaucoma. Only two eyes out of 526 (0.4%) were found to have increased eye pressure requiring treatment at 3 years post op.
Iris atrophy and pupil distortion
Since the surgery involves placing a lens close to the iris at the center where the pupil is, risk for iris atrophy or pupil distortion exist. In following up with 993 eyes undergoing ICL implantation from 1996 to 2008, iris atrophy and pupil abnormality were found in 0.2% of cases [8]. Higher incidence of iris atrophy was found in the iris-claw type Verisyse lens, 11.8% (11 out of 93 eyes) [9]. This may be skewed from being a study with smaller number of patients, but it is also not a surprise, as the Verisyse lens is fixed on the front of the iris.
So, pIOLs or LASIK?
First of all, remember that all surgeries carry risks, and that wearing spectacles is safe and involves no manipulation in your eyes.
However, if refractive surgery is something you want to go for, make sure you know the indications, benefits, risks and complications associated with each. LASIK is approved for myopia up to -11.00 D, and appropriate corneal thickness is required. Common complications include dry eye, and rare but more serious complication such as corneal ectasia can be detrimental to vision.
pIOLs are better for high myopia up to -20.00 D, does not require a thick cornea but requires healthy corneal endothelial cells and a deep anterior chamber. Complications include cataract and corneal endothelial cell loss; and, as a more invasive procedure, retinal detachment and eye infections can happen though very rare. Caution to older patients and those with higher myopia, as risk of cataract goes up significantly in these patient populations.
In terms of efficacy, both are quite good with high patient satisfaction, though LASIK achieving slightly better correction to target.
In terms of long-term safety, LASIK has been approved in the US for over 20 years whereas pIOLs for 12 years, both have been relatively safe with small percentages of complications as discussed in this article and before.
Lastly both procedures are elective and not covered by insurance; pIOL costs about $4,000 per eye, whereas LASIK about $2,000 per eye in the US.
If you are interested in refractive surgeries, make sure you go for complete eye exams and rule out eye and systemic conditions that contraindicate these surgeries. Eye doctors will recommend the appropriate procedure based on your specific eye conditions and systemic health. Make sure you follow doctors’ instructions for pre and post op care to prevent unnecessary complications.
References
- Hassaballa, M.A. and T.A. Macky, Phakic intraocular lenses outcomes and complications: Artisan vs Visian ICL. Eye (Lond), 2011. 25(10): p. 1365-70.
- Igarashi, A., K. Shimizu, and K. Kamiya, Eight-year follow-up of posterior chamber phakic intraocular lens implantation for moderate to high myopia. American Journal of Ophthalmology, 2014. 157(3): p. 532-9 e1.
- Huang, D., et al., Phakic Intraocular Lens Implantation for the Correction of Myopia. Ophthalmology, 2009. 116(11): p. 2244-2258.
- Lee, J., et al., Long-term clinical results of posterior chamber phakic intraocular lens implantation to correct myopia. Clin Exp Ophthalmol, 2016. 44(6): p. 481-7.
- Packer, M., Meta-analysis and review: effectiveness, safety, and central port design of the intraocular collamer lens. Clin Ophthalmol, 2016. 10: p. 1059-77.
- Fernandes, P., et al., Implantable collamer posterior chamber intraocular lenses: a review of potential complications. Journal of Refractive Surgery, 2011. 27(10): p. 765-76.
- Galgauskas, S., et al., Age-related changes in corneal thickness and endothelial characteristics. Clinical Interventions in Aging, 2013. 8: p. 1445-1450.
- Zhou, T.A., et al., [Mid-long term follow-up results in correction of extreme myopia by posterior chamber phakic intraocular lens]. Zhonghua Yan Ke Za Zhi, 2012. 48(4): p. 307-11.
- Benedetti, S., et al., Correction of myopia of 7 to 24 diopters with the Artisan phakic intraocular lens: two-year follow-up. Journal of Refractive Surgery, 2005. 21(2): p. 116-26.
Additional websites that are helpful:
- http://www.allaboutvision.com/visionsurgery/implantable-lenses.htm
- FDA phakic IOL page: https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/ImplantsandProsthetics/PhakicIntraocularLenses/default.htm
- https://crstoday.com/articles/2006-apr/crst0406_11-html/