Month: December 2022
Keratoconus- a creepy eye disease that affects the young
This article is also available in a podcast: https://spotifyanchor-web.app.link/e/C3O8RRhTsvb
Juan Ding, OD, PhD
The mysterious case of poor vision with contact lenses
A 38 year old guy came to see me to check his contact lens prescription. He got the final contact lens prescription from another optometrist in our practice in March, so about 8 months ago, and he could no longer see well with them. This is a red flag. In adults, prescriptions are typically stable for years. 20-40 is a stable and healthy period for the eyes, with relatively few diseases and certainly few fluctuations in refractive power of the eye. But our patient obviously has a problem despite his young, primal age. So let’s look at what’s going on.
He’s wearing biofinity Toric XR lenses. For those of you who are not familiar with it, this is a monthly disposable contact lens that corrects for high amount of astigmatism that most other regular contact lenses do not correct. Toric lens is a lens that corrects for astigmatism. Astigmatism is when the eyeball is not shaped perfectly like a soccer ball, but rather a bit like the American football, so different in terms of curvature on the two different planes. And that’s why people can get blurry vision with astigmatism and there are certain contact lenses, the toric contact lenses that can correct this. Right now his contact lens prescription is about -8 – 3.5, that means he has about 8 diopters of myopia as well as 3.5 diopters of astigmatism. As you can see that’s a lot. When I look at this previous record from March, he was wearing these contact lenses and his vision was about 20/30 with the correction. So that was not 20/20 either. And 20/20 is usually the standard healthy vision that we’re aiming for. Anyone without a notable disease of the eye should have the standard 20/20 vision, especially adults. Today his vision with the contact lenses is only 20/100 and he has over these contact lenses a very large prescription, another five diopters of astigmatism. That is really striking difference, and that should not happen with healthy eyes.
When I asked him, he reported that even when he first got the contact lenses, he was not really seeing all that well. And now it’s getting progressively much, much worse, to the point he could no longer work and it was difficult to drive. I asked him, “Are you sure you put the contact lenses in the right eye?” Sometimes patients would mistakenly switch the contact lenses for the two eyes and that can make things a little funny as obviously the two eyes will be using the wrong prescriptions for both of them. He said that he made sure of it. In the past, he did accidentally switch the two lenses and it was very blurry. He was able to recognize that and switch them back, and now this he was very sure he was using the right lens in the right eye.
I asked him to take off his contact lenses and started doing refraction again. It turned out he could not really see that well even with the new prescription. And the new prescription was markedly different than his current prescription back from March as well. So his glass prescription has also changed a lot. This is very strange. At this moment I was suspecting something funny on the surface of the eye because he does not have diabetes, which is another common cause of large refractive changes over a short period of time. A really quick way to test this is to check the red reflex on retinoscopy. I took up the retinoscopy scope, and this is a light that you can shine into a patient’s eyes and the red reflex would show up funny if there is anything irregular on the surface of the eye. However, nothing wrong showed up there.
I then took a look at his eyes under a microscope, a slit lamp. This is a lighted microscope that you can magnify and see fine details of the eye. I was looking at the surface of his eye and it looked really healthy. There was no notable dry eye. He’s got healthy tears as well. His cornea is completely clear and there’s no staining on them. There’s no opacity on the cornea.
I didn’t dilate his pupils and check the back of the eyes immediately. I could put some dilating eye drops in and check to see if there’s any disease in the middle or in the back of the eye. But I didn’t do that. With the dilation you have to put the drops in and that takes about 20 minutes for the pupils to get bigger. And patient’s eyes remain dilated for the next four to six hours. It can cause a lot of inconvenience. Obviously when it’s necessary, we have to do this. But he’s got to work afterwards and doesn’t want to get dilated.
So the next high yield exam is a corneal topography. This is a machine that draws a map, a very fine, high resolution, accurate map of the surface of the cornea that you may not necessarily see with just the magnifier or with a retinoscope. This test is quick. You just need to turn the machine on, patient looks into a bowl of concentric rings, and it takes a few seconds to take a picture for each eye. A minute later, it becomes apparent that there is something wrong going on in the corneal surface that I am not able to see with the other techniques. It is not very obvious. It is kind of subtle, but he’s got a condition called keratoconus. Figure 1 shows his corneal topography findings.
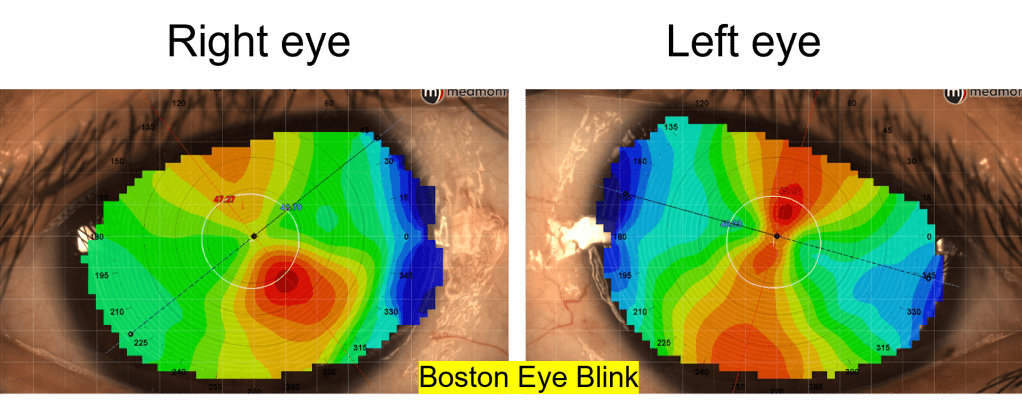
Figure 1. Corneal topography map of definite keratoconus in the right eye and possible keratoconus in the left eye.
What is keratoconus?
Keratoconus is a condition that affects the cornea of the eye, and cornea is the very surface of our eye, the clear thin membrane covering up the surface of the eye, and through that clear cornea you can see the iris, which is the colored part of the eye, as well as pupil, which is the small opening in the center of the iris. The front surface of the cornea is very important. If there’s anything irregular going on, your vision can be blurry. In keratoconus, the cornea undergoes degenerative changes through the years. It can happen very quickly over a short period of time, but it can also stay dormant for months and years. Keratoconus happens in about 1 in 700 people in the general population. So while it is not extremely common, it is also not a rare disease.
This is unfortunately a disease that affects the young people. Children as young as eight years of age can start developing keratoconus, but typically it happens in late teenage years and it can continue to get worse through the years. It happens to both eyes, but it can be asymmetrical, meaning one eye may be affected more. I’ve seen many people who have one eye completely normal 20/20 vision do not need glasses. The other eye with relatively advanced keratoconus.
But even in this apparently normal eye, if you do the corneal topographer map like what I did for the patient, you could see some problem for the normal eye. The apparent normal eye may also have sign of very mild keratoconus that’s fortunately off center- it’s often inferior, that means in the lower part of the cornea so it’s not in the visual axis. That’s why patients can see well, it’s not affecting their vision. But nonetheless, the disease is there and it may be dormant in the lifespan of a person, but it can also start progressing anytime.
Who are affected by keratoconus?
The cause of disease is still not clear, but people have seen that this runs in the family. Of course, it can happen to someone who has absolutely no family history of keratoconus, and it just starts with them. Or you can have parents with keratoconus, but the children can be completely normal. The genetics of this is not completely figured out, although some company is selling genetic tests for this condition.
It is believed that changes in the enzymes of the cornea are undergoing changes, bad changes that break down the collagen of the cornea. There are several layers of the cornea and some of these layers are fragmented and also becoming much thinner. There is sometimes a break or folds in these layers, and that also can lead to scarring and making the cornea very cloudy.
People have observed a few things that are associated with keratoconus. One of them is rubbing of the eyes, and many doctors believe that the rubbing mechanical action on the cornea itself can make it change in shape, thinner and make lose its normal property. And that certainly has its merits. Except, many keratoconus patients actually don’t rub their eyes. Some of them do, and they often have other conditions like allergic conjunctivitis. Their eyes are always itchy or dry and they feel uncomfortable and hence they always rub their eyes and that does make keratoconus worse. But many people actually rub their eyes a lot, but never develop keratoconus. This patient denies rubbing his eyes. He denies having itchy eyes or irritable eyes. And the surface of his eye as well as his conjunctiva do look pretty healthy. There’s no sign of inflammation there, so I have no reason to believe that he is lying.
Another association people have observed is that those with Down syndrome sometimes have keratoconus. Although, in my experience as a primary care optometrist, many Down syndrome patients have perfectly healthy corneas and majority of my keratoconus patients don’t have Down syndrome.
And another condition that’s associated with keratoconus is Ehlers-Danlos syndrome, a connecting tissue disorder. It kind of makes sense that their cornea would be weaker because cornea is made of collagen, which is the component of connective tissues.
Some risk factors have been proposed for keratoconus, including number #1 eye rubbing. And #2 is sleep apnea and this is an interesting one. Now with sleep apnea there is another highly associated condition, floppy eyelid syndrome. These patients’ eyelids are pretty loose. And when they sleep, they sometimes can inadvertently flip their eyelids and their cornea can be exposed to the pillowcase, resulting in corneal injury and eye pain in the morning. So connective tissue disorders may be the underlying cause of floppy eyelid syndrome as well as sleep apnea, and that could also be the underlying cause of keratoconus.
Retinitis pigmentosa can also be a risk factor for keratoconus. This is a condition that I will talk in details another time.
Why is keratoconus sometimes missed by eye doctors?
It is not easy to diagnose keratoconus, especially in the early stage. Like I mentioned, I try using retinoscopy and that’s one way to diagnose keratoconus. Typically you would see a scissor reflex when you do the retinoscopy procedure. There are two lines crossing with each other. However, that may happen in intermediate or above level of keratoconus. In early stage it may not show up that well.
Other methods include a slit lamp exam. Sometimes you can see folds in the deeper layer of the cornea. Sometimes you can see scarring and obviously that’s a much later stage and patients typically already see poorly before that. So that’s not really useful to diagnose early keratoconus. Sometimes you can see thickened nerves. Corneal nerves are typically not obviously visible even with the magnifier, but in keratoconus, for some reason the coroner nerves can be thickened. However, this is not a specific test for keratoconus because some normal people can have thick corneal nerves. Sometimes people can see a ring that is an iron deposit present within the epithelium of the cornea around the base of the cone. But it is also not always seen, especially those with early keratoconus.
People often classically cite Munson sign as a sign of keratoconus. That is a protrusion of the lower eyelid in downgaze, because in advanced keratoconus the surface of the cornea becomes almost like a cone, and so you can see that when people look down with that cone touching their eyelid, that is advanced keratoconus. You certainly do not see that in the early form.
So many of these are helpful, but none is the definitive sign of keratoconus, or they’re often not present or not obvious in early keratoconus.
To diagnose keratoconus, you really need to have high clinical suspicion and order that corneal topography test. This test is highly sensitive and it does show keratoconus much earlier than many of the other clinical exams. Classically in a corneal topography map view you will see steepening, which is usually indicated with red color whereas normal curvature is indicated with the green color. If you see the red color in the lower part of the cornea, that’s highly suggestive keratoconus. In early keratoconus, though, that redness may not be very obvious, and you have to rely on the asymmetry of the steepening of the cornea from the upper part of the cornea as well as the lower part.
In my patient, you will see that he has a lot of corneal astigmatism. So there’s redness both from the upper as well as lower part, but the lower part of the map is much more steepening than the upper part (Figure 1). This asymmetry is also a characteristic to differentiate from a regular corneal astigmatism, that would be equal amount of steepening from both the upper and lower that would be symmetrical (Figure 2) and that would not affect vision as much. And patients typically would see well with glasses correction and obviously with the contact lenses they would see well. A corneal map of more advanced keratoconus is shown in Figure 3.

Figure 2. Corneal topography map of regular astigmatism. This patient has high degree of astigmatism, but it’s regular, hence good vision with glasses. Note the symmetry between the red areas for the upper and lower halves in both eyes.

Figure 3. Corneal topography map of a patient with intermediate to advanced keratoconus. Note the red area is only evident in the lower half of the cornea, that is, the marked asymmetry between upper and lower halves in both eyes.
The corneal topographer in our practice can only capture map of the front surface of the cornea. There are some topographers that are able to map the back surface of the cornea as well. In keratoconus, it is observed that the earliest changes actually happen to the back surface of the cornea, before any visual symptom even shows up. If you go for a LASIK surgery evaluation, they will use this type of corneal topographer, because LASIK surgeons really want to catch the most hidden form of keratoconus as it’s a contraindication of LASIK surgery, more about this later.
Another reason eye doctors won’t think twice when giving out a new stronger prescription to a young person is the myopia epidemic. Myopia progression can produce the similar phenotype with kids updating their glasses every 6 months. Both conditions affect young people and myopia is so prevalent these days. Please check out my articles on myopia and myopia control. Sadly, myopia progression and keratoconus can certainly happen to the same person.
Patients with keratoconus typically have a history of good vision with glasses, just like those with myopia. Gradually their glass prescription changes over the course of years, until eventually, even with very high prescription of glasses they could not see well. They would turn to soft contact lenses that would work well for a period of time, but then vision may get worse again, until eventually the diagnosis of keratoconus is made.
What are the treatments of keratoconus?
And that’s the time when we should address this issue. And not just treat the symptoms, but actually treat the disease itself. Although this can be a degenerative condition that progresses overtime, there’s no inflammation associated with it. So anti-inflammatory treatment or medication will not be able to help in this condition.
The treatment of keratoconus comes in several different ways. First, we want to address the underlying cause. Without the treatment, keratoconus can be progressive, so early diagnosis is key. Once you diagnose the condition, you can start a treatment called corneal cross- linking to strengthen the cornea and stop the disease from progressing further. This procedure was approved by the FDA in 2016, so not that long ago, but it is the only way that can actually stop the disease from progressing. Note it does not reverse the disease, so it does not make the cornea better, or make the vision better. Patients will still need contact lenses and glasses to see better after the procedure. The cornea cross linking procedure really strengthens the cornea and renders the corneal stable from undergoing further degenerative changes over time. In this procedure, the corneal epithelium is taken out first and you would soak the cornea with drops of riboflavin. Then the cornea is exposed to UV light for 30 minutes. During this process the collagen inside the cornea will cross-linked with each other, therefore rendering the structure more stabilized. After crosslinking, when the eyes are stable, you can use contact lenses and glasses to see better. There will not likely be further change of prescription after this procedure.
Vision in keratoconus often cannot be corrected with glasses because the surface of the cornea itself is irregular. Regular soft contact lenses also cannot correct vision to a satisfactory level. Again, because any soft contact lenses put on the eye will drape over the irregularity. So the only way that allow more than mild keratoconus patients to see a little better would be a hard contact lens, whether it’s a small hard corneal lens, called a gas permeable (GP) lens, or a bigger hard lens called the scleral lens. These hard lenses will be able to mask the irregularity of the cornea and provide clearer vision. I have prescribed a lot of both types of lenses to keratoconus patients which make them see better again. Just yesterday a patient told me ‘I have never seen this well for a long time”, after he tried on a special GP lens.
The corneal gas permeable lenses are small, clear plastic contact lenses on the surface of the cornea, so it covers the black part of the eye only, and it can move freely whenever you blink. There’s a tear layer behind the lens as well as in front of the lens, therefore masking the irregularity of the cornea. It’s relatively easy to put in and take out, and easier to care for, but in the beginning of using the lens, many patients reported their eyes hurting with foreign body sensation, especially with blinking. And that’s understandable, because after all, you’re having a hard piece of plastic inside the eye that certainly is not comfortable. Fortunately, most patients get used to them after a few weeks of using the contact lens.
Scleral lenses are much bigger contact lenses. They are sort of like a small bow that hovers over the entire eye, so it actually touches on the white part of the eye. Therefore it does not hurt as much. In fact, it is quite soothing. You almost don’t feel that you have a lens inside the eye. You would fill the bowl of the scleral lens with preservative free saline, so from that aspect it is soothing to the surface of the eye. This lens is comfortable. It also corrects the irregularity on the surface of the cornea. However, the disadvantage is that it is much more expensive and it is a little more difficult to care for. And it is also more difficult to learn how to use it as you have to use a plunger to apply the contact lens inside the eye as well as the plunger to take it out. So the learning curve is a bit steep for patients.
As with any contact lenses, the corneal gas permeable contact lenses as well as the scleral lenses need to be carefully cared for and patients should never sleep in these contact lenses, they should always take them out before going to bed and soak them into the correct disinfectant solution and to be used again the next morning. Before touching the contact lenses, patients should always wash their hands with soap and water and make sure not to touch the lens with dirty hands. Patients should not go swimming, taking a shower or sleep in contact lenses.
Medical treatment sometimes is needed. A complication can sometimes develop in keratoconus called acute hydrops, this is a condition where a break develops in the inner layer of the cornea, allowing the fluid inside the eye to enter into the corneal stroma, causing severe edema and thickening, light sensitivity, decreased vision, tearing and pain. And this needs to be managed acutely because Hydrops can lead to corneal scarring. Providers will need to try to manage the pain and swelling. We can give patient a dilating eye drop that reduces the pain. We can give patient sodium chloride 5% ointment, which can reduce edema and improve vision a bit. It may take several weeks for Hydrops to completely clear. The patients may need to use this ointment for weeks or months before it finally resolves.
Unfortunately, sometimes advanced cases can occur. Corneal scarring can occur that no contact lenses will be able to restore vision, and to that end a corneal surgery needs to be done. A new cornea transplant can be placed in to replace the keratoconus cornea that has scarring.
Why is keratoconus an emotional eye disease?
I think keratoconus is a frustrating disease. It affects young people who have been seeing well in first two decades of life. And slowly their vision starts to get worse and this change, especially when early, is often missed. So they end up going to the eye doctor’s office a lot with multiple pairs of glasses with constantly changing contact lens prescription. And with frustration that their vision continues to get worse, if lucky and it is diagnosed early and cross linking is done, the cornea can be stable and hopefully patients can see much better to a normal level with the proper contact lenses or glasses, but many of the keratoconus patients need to use specialty contact lenses for all their life. To them, contact lenses are not an option. They have to use them simply because glasses will not make their vision good enough. They have to take care of the contact lenses all their life. That is a serious commitment. You have to follow all the rules. They’re not really good candidates for LASIK surgery. And in fact, sometimes latent keratoconus can become pronounced after a LASIK surgery procedure. I have seen multiple patients who develop keratoconus after LASIK surgeries. Although nowadays people are starting to do LASIK surgery together with cross linking and this may hold to be a promising procedure for keratoconus patients in the future that they may have surgery to correct their vision and do not have to worry about complications to their cornea.
Conclusion
To recap, early detection and diagnosis of keratoconus is really key in managing this disease. Once diagnosed, crosslinking procedure should be recommended. Even though most keratoconus progression happens before 40 years of age, I have seen patients that are progressing well after 45 years of age, so a cross linking procedure should be highly recommended to any patient if it’s still progressing, no matter their age. Hopefully keratoconus patients in this day and age can be diagnosed early enough with early intervention to prevent the need of significant corneal scarring and corneal surgeries, and hopefully glasses and contact lenses are all they need. Any young person with unexplained vision reduction should have the benefit of taking a corneal topography image to rule out keratoconus.
