[1]Yam JC, Zhang XJ, Zhang Y, et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children: The LAMP2 Randomized Clinical Trial. JAMA. 2023;329(6):472–481. doi:10.1001/jama.2022.24162
[2]Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113: 2285e2291.
[3]Louis Tong, Xiao Ling Huang, Angeline L.T. Koh, Xiaoe Zhang, Donald T.H. Tan, Wei-Han Chua, Atropine for the Treatment of Childhood Myopia: Effect on Myopia Progression after Cessation of Atropine, Ophthalmology,vVolume 116, Issue 3, 2009
[4]Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119:347e354
[5]Chia A, Chua WH, Wen L, et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157:451e457.e1.
[6]Yam JC, Li FF, Zhang X, et al. Two-year clinical trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2020;127: 910e919
[7]Yam JC, Zhang XJ, Zhang Y, Wang YM, Tang SM, Li FF, Kam KW, Ko ST, Yip BHK, Young AL, Tham CC, Chen LJ, Pang CP. Three-Year Clinical Trial of Low-Concentration Atropine for Myopia Progression (LAMP) Study: Continued Versus Washout: Phase 3 Report. Ophthalmology. 2022 Mar;129(3):308-321. doi: 10.1016/j.ophtha.2021.10.002. Epub 2021 Oct 7. PMID: 34627809.
[8]Wang W, Zhang F, Yu S, Ma N, Huang C, Wang M, Wei L, Zhang J, Fu A. Prevention of myopia shift and myopia onset using 0.01% atropine in premyopic children – a prospective, randomized, double-masked, and crossover trial. Eur J Pediatr. 2023 Jun;182(6):2597-2606. doi: 10.1007/s00431-023-04921-5. Epub 2023 Mar 22. PMID: 36944782.
The flu season is upon us now. Many people are getting sick, coughing, sneezing, having a fever, and sometimes developing pink eyes, also known as infectious conjunctivitis. There are also people who develop pink eyes without any other cold symptoms. Pink eyes are miserable, with redness, pain, discharge and sometimes blurry vision. They look awful, you cannot go to work as people will ask questions, and rightfully so as infectious conjunctivitis is quite contagious.
So how can you get well quickly? Patients often go to doctors asking for drops that will ease the pain and make them look normal again.
What can eye doctors give patients to make their pink eyes better?
Many primary care doctors will give patients antibiotic eye drops. Eye doctors, however, are trained not to do that automatically. You see, not all pink eyes will respond to antibiotic drops. In fact, we are taught that most pink eyes are caused by viral infections, which will not respond to antibiotics, and using antibiotics in this situation will contribute to antibiotic resistance.
So how to tell bacterial from viral infections? It’s not possible for a patient to do this. It’s actually difficult even for eye doctors. There are certain characteristics that are classical for viral vs bacterial, but many features are overlapping between the two. The only accurate way is to culture or test specifically for the pathogen. Unfortunately, this is almost never done in any eye doctors’ offices. I can imagine the reason to be related to cost, and most pink eyes get better even without treatment anyways.
There is a product similar to a quick strep throat swab test, that checks if the pink eye is from adenoviral infection, which is considered to be the most common virus to cause pink eyes. If your eye swab tests positive for adenovirus, then the pink eye is confirmed to be from this virus, and no treatment is going to be needed, as this virus does not respond to antibiotic drops, nor to the antiviral drops currently available. So just use artificial tears and cold compress to make yourself a bit comfortable while waiting it out.
However, even though the product is there, the adenoviral testing is still not widely used in most offices. Cost being one reason, and the other reason is that it tests for only one thing. If you test negative for adenovirus, then you don’t know whether it’s another virus or it is a bacterium, or fungus, so that does not help with the treatment.
So now there is a new study [1] that checked for any possible pathogen for pink eyes. They collected eye and nose swabs of 52 adult patients with pink eyes from 4 sites in the US and 1 site in Israel, and did DNA sequencing in these samples and compared the sequence to all the currently known DNA sequences of microorganisms. This way, anything that caused the pink eye is being looked at, not just adenovirus. The results are interesting.
First, they did find that most of the infections are from virus rather than bacteria. 54% were from viruses and only 8% from bacteria. 35% they were not able to identify any pathogen (could be due to some of the patients already started on antibiotic drops, or technical difficulties, or the presumed diagnosis of infectious conjunctivitis is just wrong). And the rest (3%) are from fungus.
This is great confirmation that most pink eyes are viral, but I am disappointed that they included 33% of patients who started antibiotics before sampling, and you have 35% samples tested negative for any pathogen. This looks suspicious, what if these are rightly diagnosed as bacterial conjunctivitis and treated successfully before sample collection, hence the negative hit in pathogen database. If that’s the case, then the bacterial etiology is not as infrequent as we think. They should have analyzed the 35% negative results in depth, especially cross referencing to those who took antibiotics beforehand. I’m surprised this slipped through the reviewers as well as authors.
Still, their findings are useful and eye opening as they debunk certain myths around infectious conjunctivitis.
We are taught that one way to differentiate bacterial vs viral is that bacterial infection causes mucopurulent discharge vs virus causes watery discharge. But this study finds that while all the bacterial conjunctivitis produced mucopurulent discharge, 17 viral conjunctivitis patients also presented with mucopurulent discharge. So out of the 28 with viral etiology, that is 61% of all viral conjunctivitis show mucopurulent discharge. This tells us that if a person has watery discharge, it’s most likely not due to bacteria, but if they have mucous discharge, you cannot say for sure that they have bacterial infections. This also implies that bacterial conjunctivitis is probably over-diagnosed, as doctors may use the texture of the discharge as a criterion.
Another myth is that itchy eyes equal allergies, and infectious conjunctivitis produce pain or discomfort, rather than itchiness. Their study found that 64% of patients report eye itchiness. So this is an overlapping symptom of infection with allergy. You cannot conclude a conjunctivitis is due to allergy just because patients feel itchiness.
Third myth is that viral rather than bacterial conjunctivitis is associated with swollen lymph nodes. In the study, only 4 out of the total 52 cases show preauricular lymphadenopathy (PAN). This is something I see in clinic frequently. Most viral conjunctivitis does not present with PAN.
We are taught that most viral conjunctivitis is caused by adenovirus. In this study, 13 of 28 viral cases (46%) were indeed due to adenovirus. The other viruses identified included: 3 with human coronavirus 229E, 1 with SARS-CoV-2, 3 cases of herpes simplex virus type 1 (HSV-1), 2 cases of varicella-zoster virus (VZV), and 2 cases of Epstein-Barr virus, 1 case was positive for human metapneumovirus.
Both human coronavirus 229E and human metapneumovirus commonly cause cold and sometimes pneumonia. The same with adenovirus, which seems to have a predilection for conjunctival infection, while also causing common cold and sometimes pneumonia. There is no treatment for these viruses, and their conjunctival infections typically are self-limited.
Therefore, in viral conjunctivitis, no antibiotic eye drops should be given.
HSV and VZV can cause pink eyes as well. Antibiotic eye drops will not work on these herpes viruses so should not be given. But unlike other viral causes, there are anti-viral medications that can be used to treat HSV and VZV. Without other concomitant presentations, such as findings in the cornea and on eyelid skin, it can be difficult to differentiate HSV or VZV from other viral causes. Given HSV and VZV only represent a small percentage of the viral conjunctivitis, it may not be worthwhile treating every pink eye with antivirals.
Therefore, we typically don’t treat pink eye with antivirals if there is no involvement of the cornea or other tissue of the eye.
How about bacteria?
Bacteria were identified in 4 patients (8%), including Haemophilus influenzae, Fusobacterium nucleatum, and Streptococcus pneumoniae.
Haemophilus influenzae and Streptococcus pneumoniae are known human pathogens to cause respiratory tract infections, as well as more invasive systemic infections. When these cause conjunctivitis, most antibiotic eye drops will successfully treat the disease.
Fusobacterium nucleatum is actually a commensal bacterial living in the oral cavity and rarely found elsewhere in the body. However, it can cause oral infections, GI disorders, problems with pregnancy, rheumatoid arthritis and Alzheimer’s disease, among many [2]. It is a Gram-negative, anaerobic bacterium, so most of the antibiotic eye drops should take care of it.
So yes, if we are certain the pink eye is caused by bacteria, then antibiotic eye drops are warranted.
Fungus was identified in 2 patients (4%), Rhizopus oryzae, which is a mold found in soil and food, an opportunistic pathogen of humans causing mucormycosis. Fortunately this is quite rare for pink eyes, because the treatment would have been an anti-fungal eye drop.
So in summary, most of pink eyes in adults are caused by viruses, which are often self-limited and non-responsive to antibiotics (or even antivirals that we currently have), so it is wise not to jump into antibiotics automatically. However, it is not easy to differentiate bacterial vs viral causes, and new research further made this point. Maybe one day there will be a diagnostic panel that detects multiple viruses and bacteria at the same time quickly to help doctors with more accurate diagnosis and proper treatment. Until then, we do what we do most of the time, to comfort and to let the body heal with time.
We all know that the sunlight is the best light to prevent and control myopia in children. I have previously published multiple media items to talk about this and you can view them here. Indeed playing outside is the best way to prevent myopia. However, given the modern lifestyle, it is inevitable that we are still spending majority of the awake time inside a house, be it home, school, work or even entertainment. What can we do to reduce myopia while inside the house?
The key is to ensure that children have sufficient ambient light when staying indoors [1,2], including doing all activities, such as studying, eating, having fun, that is, except for sleeping at night.
If you can afford a glass house such as the one below, then you are all set. The sun will be your light source. It’s like you are living outside all the time. No one will develop myopia in such a house, ever.
However, as dreamy as this house may be, you and I most likely will never get to live in one, so we have to resort to having good lamps.
Living in New England, most of the houses here are old, without the floor to ceiling windows you see in modern homes, and winter here is basically 6 months long with extended dark nights. Mind you, it gets dark at 4 PM, so when you get home from work or school, you will not have any natural light to do myopia-preventing outdoor activities. This will be a good time to crack up your home light intensity. The brightest light indoors is still several orders of magnitude weaker than outdoor sunlight. So never worry that your light may be too bright. On the contrary, always worry that your light is too dim.
Most homes will use some or all of the lighting sources: desklamp, floor lamp or ceiling lamp. I will provide some guidelines for how to choose a good one for myopia control for each of these.
Desk lamp
1. Sufficient brightness
Desk lamps should provide sufficient brightness to ensure that reading materials such as books, documents, and screens are clearly visible and reduce eyestrain. Usually, the suitable reading brightness is about 300 to 600 lumens.
2. Good color accuracy
Choose desk lamps with a high color rendering index (high Ra) as they can render colors more accurately and reduce visual fatigue. By definition, Ra under natural light is set as 100. When you choose a desk lamp, try to choose Ra95 or above, so that the color accuracy is closer to that under natural light.
3. Good uniformity of illumination
Make sure the light from the desk lamp is evenly distributed and does not create noticeable shadows or glare. The smaller the variation in lighting, the less likely it is that the pupils will dilate or constrict, which can lead to visual fatigue.
4. Comfortable color temperature [3, 4]
The color temperature of a light is an indicator that describes its color appearance, usually expressed in units of Kelvin (K). Different color temperatures will produce different visual effects. Here are some differences between different color temperatures:
Lower color temperatures (2700K – 3000K): Lower color temperatures typically appear as warmer tones, similar to yellow or orange light. This color temperature is warm and comfortable, suitable for casual environments.
Medium color temperature (3500K – 4500K): Medium color temperature usually appears as natural white or natural daylight color. This color temperature is fresh and neutral, which is more suitable for studying. It helps improve alertness and concentration.
Higher color temperature (above 5000K): Higher color temperature appears as cool colors, similar to a bluish white light. This color temperature is typically used in environments that require a high degree of lighting and visual precision, such as operating rooms, laboratories and workshops. Higher color temperatures can increase alertness and concentration, but may feel cold when used in a home environment.
In addition, the color temperature of the lights can also be adjusted between different activities and time periods to suit different needs.
For example, you can use a medium color temperature when studying during the day; and at night, if you plan to read a book before going to bed, you can adjust the color temperature to a lower color temperature to help you relax and get ready for asleep.
Some desk lamps can have settings to adjust between different color temperatures as well as brightness of the light, which are helpful.
5. Ability to adjust brightness
Even though it is beneficial to prevent myopia by using as bright a light as possible, in some cases, you may find it difficult to tolerate bright light, such as when you have dry eye syndrome, conjunctivitis, or migraine headaches. Turn down the brightness if you suffer from these conditions.
6. Blue light
There is a lot of debate about blue light for eye health. Blue light is part of the natural visible light spectrum. A normal dose of blue light exposure is good for the eyes, circadian rhythm, and a happy mood, but excessive exposure is bad [5].
The visible light spectrum of sunlight is a continuous spectrum, including blue light and all the way to red light. Compared with natural light, the spectrum of many LED lights contains a disproportionately high amount of blue light. When you choose desk lamps, try to choose light bulbs with a continuous spectrum and no excessive blue light.
7. Avoid flickering
Desk lamps should not produce significant flicker, as flickering light sources may cause eye discomfort.
8. Proper positioning, height and angle
Place the desk lamp in a suitable position to ensure that the reading material is illuminated without the light shining directly into the eyes. Avoid light shining on the screen or reflect onto your eyes. Some desk lamps have adjustable arms, lampshades, diffusers or beam angles that allow you to adjust the direction and range of light as needed.
9. Additional functionality
Some modern desk lamps come with remote controls, touch controls, or smartphone app controls for easier operation and adjustment. These have nothing to do with myopia control and can be selected according to personal preferences.
10. Energy efficiency
Choosing energy-efficient desk lamps can reduce energy consumption, help save money on electricity bills, and be greener on the environment. LED desk lamps generally have high energy efficiency. Although our focus is on preventing myopia, it would be better if it could also save energy.
Although desk lamps are the direct source of light for children to study, the lighting of the environment in which children live and play is also important. When we are outdoors, the entire environment is bright, not just the 40 centimeters in front of our eyes.
So while using a desk lamp, you can also consider turning on a floor lamp or ceiling lamp. The considerations for selecting these lamps are similar to those introduced before for desk lamps, but there are a few additional considerations.
∎For ceiling lights, good design and shading should also be considered: tryto prevent the light from directly entering the eyes.
∎For floor lamps, in addition to good design and shading, you can also consider the appropriate height and whether the light direction can be adjusted: Some floor lamps have adjustable arms or lampshades, allowing you to control the direction and range of light.
Good indoor lighting is necessary not only in the study room, but the entire environment should be as bright as possible. For example, install a good ceiling light above the dining table so that family can enjoy food in a nice a bright environment. If you are like me, you would spend a good amount of time eating dinner every day. Many families have a sunroom for children to play in, which is a fantastic idea. If children are playing or watching TV in the living room, it will be beneficial to add ceiling lights or additional floor lamps to increase the brightness of the environment.
In summary, the best indoor lighting for myopia control is bright illumination as well as a few other perks, possibly utilizing multiple light sources throughout the house. Ideally this is in addition to the out door activities, not instead of them.
References:
[1] Jiang X, Kurihara T, Torii H, Tsubota K. Progress and Control of Myopia by Light Environments. Eye Contact Lens. 2018 Sep;44(5):273-278. doi: 10.1097/ICL.0000000000000548. PMID: 30048342
[2] Landis EG, Yang V, Brown DM, Pardue MT, Read SA. Dim Light Exposure and Myopia in Children. Invest Ophthalmol Vis Sci. 2018 Oct 1;59(12):4804-4811. doi: 10.1167/iovs.18-24415. PMID: 30347074
[3]Weitbrecht WU, Bärwolff H, Lischke A, Jünger S. Wirkung der Farbtemperatur des Lichts auf Konzentration und Kreativität [Effect of Light Color Temperature on Human Concentration and Creativity]. Fortschr Neurol Psychiatr. 2015 Jun;83(6):344-8. German. doi: 10.1055/s-0035-1553051. Epub 2015 Jun 22. PMID: 26098084.
[4]Chao Wang, Fan Zhang, Julian Wang, James K. Doyle, Peter A. Hancock, Cheuk Ming Mak, Shichao Liu, How indoor environmental quality affects occupants’ cognitive functions: A systematic review, Building and Environment, Volume 193,2021,107647,ISSN 0360-1323,https://doi.org/10.1016/j.buildenv.2021.107647.
[5]Wahl S, Engelhardt M, Schaupp P, Lappe C, Ivanov IV. The inner clock-Blue light sets the human rhythm. J Biophotonics. 2019 Dec;12(12):e201900102. doi: 10.1002/jbio.201900102. Epub 2019 Sep 2. PMID: 31433569; PMCID: PMC7065627.
Yes, low dose atropine can lower myopia risk if used in children without myopia in this Hong Kong study. However, even without it, 47% of the studied children did not develop myopia after 2 years. In those using 0.01% atropine, 54% did not develop myopia, and in those using 0.05% atropine, 72% did not develop myopia. A dose dependent effect of myopia prevention can be inferred. But whether to use atropine or what dose to use should be an individualized process.
This article is also available in an audio podcast format in case you want to give your eyes a break. Click here to listen.
Official full text below
Recently, the University of Hong Kong published a paper [1] to study whether two different concentrations of low-dose atropine can prevent the development of myopia for children whose eyes are not yet myopic. This is a randomized double-blind study involving more than 400 children aged 4-9 years old with 0-1.00 diopters of hyperopia. About 1/3 received placebo, 1/3 used 0.05 % atropine once daily, and 1/3 used 0.01 % atropine eye drops once daily for two years, and the development of myopia was observed in these children. The study found no statistically significant difference using atropine 0.01% compared with placebo. In contrast, atropine at a concentration of 0.05% was able to delay the progression of myopia. After this article came out, many people had doubts. Wasn’t it shown that atropine at a concentration of 0.01% can control the growth of myopia? Why can’t it play a role in preventing myopia? So should we not use 0.01% atropine at all, but should use 0.05% instead?
To explore this issue, we need to understand the history of atropine used to control myopia.
It was discovered decades ago that 1 % atropine (note the high concentration) could slow down the progression of myopia. However, relatively high-quality evidence, such as a randomized, double-blind clinical study, was not published until 2006. In 2006, a clinical study conducted in Singapore confirmed that 1 % atropine was used for 2 years to effectively control myopia, reducing myopia by 7 7% [2]. Of course, its side effects are also very significant. 1% atropine is a common drug used to dilate pupils for fundus examination or for cycloplegic refraction. It can effectively dilate the pupils and completely paralyze the ciliary muscle of the eyes, so the eyes will be very light sensitive and blurry when looking at near objects. This side effect makes it unrealistic to use 1% atropine to control myopia. Almost no one can tolerate such side effects, especially considering that myopia control is done over many years, due to myopia progression naturally stops only between the ages of 16 and 18. Another disadvantage of 1% atropine for myopia control is that myopia progression actually rebounded remarkedly after discontinuation [3].
Later, scholars in Singapore did more randomized double-blind studies [4], they studied whether lower concentrations of atropine besides 1% atropine can also play a role in controlling myopia, which may have less severe side effects. They studied concentrations at 0.5%, 0.1%, and 0.01%. In this study, scholars found that the effect of atropine on controlling myopia is a concentration-related. That is to say, the higher the concentration, the better the effect of controlling myopia. But the side effects are also dose dependent. Another result that surprised them is that 0.01%, which is equivalent to diluting 1 % atropine 100 times, can still play a role in controlling myopia. And this concentration of atropine has almost no mydriatic (pupil dilating) effect and side effects. This study was also observed for two years.
At the third year, all children stopped using atropine, and the researchers wanted to see whether myopia would continue to grow. They found that after stopping the relatively high concentrations of atropine (0.5 % and 0.1 %), the myopia rebounded, that is to say, the speed of myopia progression increased faster than average myopic children. But surprisingly the 0.01% concentration of atropine showed no such phenomenon of rebound [5].
The study found that the side effects of atropine at a concentration of 0.01% are very low. Although there are some side effects of mydriasis and loss of accommodation, the vast majority of children are not disturbed, and they can still see normally.
This result suggests that although the concentration of 0.01% atropine is very low, it can effectively control myopia, and the side effects are also the lowest. It is conceivable that the safety is also the best. After this research was published, many countries in Asia began to use 0.01% atropine to control myopia in children. At the same time, people started to steer away from the relatively high concentration of atropine (a concentration greater than 0.1 %), because these high concentrations may not only have worse side effects, but also rebound after discontinuation.
However, at this time, there is no research on concentrations in between 0.1% and 0.01%. Will they also be effective in controlling myopia? How about the side effects? What about myopia rebound after discontinuation?
To answer these questions, researchers at the University of Hong Kong conducted research on this issue. They recruited children who had already developed myopia and randomly assigned them to placebo, 0.01%, 0.025%, and 0.05% concentrations of atropine once a day. Their research also found that the effect of atropine on controlling myopia has a dose dependent effect, and the higher the concentration, the better the effect of controlling myopia. The effect of atropine 0.025% and 0.05% in controlling myopia is better than that of 0.01% [6]. Reenforcing previous research, compared with placebo, atropine at a concentration of 0.01% can still control myopia. The researchers also tested the children’s accommodation and how pupil size was affected by these different concentrations of atropine. It turns out that it is also related to the concentration, that is to say, the higher the concentration, the greater the side effects. However, even atropine at a concentration of 0.05% is still tolerated by most children.
After the two-year study, they also stopped using the drug for a year to see if the myopia would rebound. This result is also related to the concentration of atropine. If the concentration is slightly higher, such as 0.05%, the rebound will be slightly more. Of course, this rebound is much smaller than the rebound of atropine with a higher concentration such as 0.1%, 0.5% and 1%. The lowest rebound is still 0.01% [7].
These results are actually quite consistent with the previous results in Singapore. Generally speaking, we know that the higher the concentration of atropine, the better the effect of controlling myopia, but even at a concentration of 0.01%, it is already effective. In terms of side effects, atropine at a concentration of 0.05% or lower are relatively easy to tolerate, and more than this concentration will be worse, and more children will not be able to tolerate it. Therefore, it is generally believed that atropine with a concentration of 0.05% or lower should used, and atropine with a higher concentration is not recommended. In particular, there are other means to control myopia, such as orthokeratology lenses, peripheral defocused spectacles, and soft multifocal contact lenses, so it is not necessary to insist on a high-concentration atropine, which will reduce quality of life. Since the long-term safety of atropine is still under study, it is important to minimize drug exposure, using a relatively low concentration and with the shortest duration possible. The rebound phenomenon after discontinuation also needs attention, as there may be many children who will not be able to use atropine all the years until they are 18. From this point of view, 0.01% concentration of atropine is still a good choice.
These previous studies were conducted on children who had already developed myopia. But more and more parents are asking, since low-concentration atropine can effectively control the growth of myopia, can I use it when my child is not yet myopic, so as to prevent my child from developing myopia, maybe he will never develop myopia?
The current study by the University of Hong Kong helped us answer this question. The data of this study tell us that the use of 0.01% and 0.05% atropine to prevent the development of myopia is relatively safe, and the side effects in these children are also relatively low, and most children can tolerate it. The effect of 0.05% concentration of atropine is significant. But they also found that 0.01% atropine was not much different vs controls. So should 0.01% concentration of atropine be abandoned?
We have to analyze this issue with logic. Though this new study unfortunately did not include the 0.02% concentration, a trend can be seen from the data that the effect on the prevention of myopia is dose dependent. Atropine at a concentration of 0.01% was actually better than placebo (Figure 1), though this result did not reach statistical significance. Myopia developed in 45.9% of the children given atropine 0.01% compared with 53% of the children given the placebo.
Figure 1. Myopia prevention by atropine. In the beginning, none of the children had myopic (the value was 0). As time went by, more and more children developed myopia. But the children who received 0.05% atropine had the lowest rate of myopia. The blue line is the placebo group, the black line is the 0.01 % atropine group, and the orange line is the 0.05 % atropine group. The chart comes from reference [1]
I think the results of this study are quite consistent with previous studies on myopic children, that is to say, the higher the concentration, the better the effect of atropine on controlling or preventing myopia. This is straightforward, logical, and supported by a lot of previous data. So the 0.01% is just a dose that is very low, that in certain population the effect is not significant enough. And this population happens to be one that even without any intervention, myopia does not develop in half the children, as shown by the placebo group. That is to say, even in the group of children who received atropine at a concentration of 0.05%, perhaps half of the children did not need to use it at all and would not develop myopia.
On the other hand, though 0.05% atropine is effective, it is not 100% effective. After two years of intervention, approximately 28.4% of children in the 0.05% atropine group were still myopic. So it is clear that 0.05% atropine can indeed reduce the risk of developing myopia within two years, but it cannot completely avoid the occurrence of myopia.
This is the conclusion of the research. There is naturally a big difference between real life and research. In the study, a child is randomly assigned to a treatment regimen for a time set by the study, say in this case two years. In real life, of course, it is impossible to apply a fixed method to a child, regardless of the effect of the method itself over years. For example, in real life, we may give a child 0.01% concentration of atropine to control myopia. If it is observed that the control effect is not very good, we will switch to other methods, such as increasing the concentration of atropine, or changing to orthokeratology lenses or soft multifocal contact lenses, instead of continuing to use the same method mechanically. Therefore, the enlightenment brought to us by a study is mainly the effect and safety of the treatment method itself. Based on this information, we can apply the methodology to treat patients. It is not an automatic copying of the research.
What we know so far is that the safety of low-concentration atropine between 0.01% and 0.05% is relatively good, and most children can tolerate the side effects. In children who are already myopic, it can control myopia, and the higher the concentration within this range, the better the control effect. We also know now that even in non-myopic children using these concentrations of atropine can reduce the risk of myopia development, a similar dose dependent effect can be inferred. But this does not mean that when children are not nearsighted, 0.05% concentration of atropine should be used to prevent myopia automatically. Consider that 47 % of children do not develop myopia within two years even without any medical intervention. If 0.05% concentration of atropine is blindly given to every child, this will increase unnecessary drug exposure to nearly half of the children.
For those children whose parents are myopic, and whose eye axial growth is relatively fast and hyperopia is declining rapidly, if the parents and children have a strong motivation to prevent the development of myopia, 0.05% can be considered in this scenario. But for a child with relatively stable hyperopia and normal eye axial growth, it is not necessary. It is safer to observe regularly and intervene only after changes are detected.
Even after children develop myopia, what kind of concentration to use is a personalized treatment process. Atropine at a concentration of 0.01% can indeed reduce the rate of myopia increase, which has been confirmed in many clinical trials. A more reasonable consideration is to use 0.01% concentration of atropine to control after the development of myopia, and observe regularly for six months to one year. If the effect is not good, then increase the concentration to 0.05% , add/or use other controls model. Because there are indeed many children who can get effective myopia control after using 0.01% concentration of atropine alone, with the least rebound effect and side effects. If you use a relatively high concentration directly without trying a low concentration first, you will not know whether the child can effectively control myopia with only a lower concentration, which is not conducive to reducing drug exposure.
As a parent, you can communicate with the doctor to formulate a personalized treatment plan that suits your child, instead of blindly following the trend and using atropine with a relatively high concentration for control.
To summarize the existing research results of atropine in controlling myopia: atropine can effectively control the growth of myopia, and this effect is related to the concentration, the higher the concentration, the better the effect. However, the higher the concentration, the greater the side effects, and the more rebound after discontinuation. At present, it is found that 0.01%, and 0.025% and 0.05% concentrations of atropine can effectively control the further growth of myopia. And their side effects are acceptable to most children. For prevention of myopia, 0.05% concentration of atropine can also be considered. Atropine at a concentration of 0.01% has no significant difference from placebo in the prevention of myopia in one study so far. But the current study is limited to children in Hong Kong, and the follow-up is only two years. In fact, for an individual child, what method to use to prevent or control myopia should be a personalized plan for the child and their family.
References
[1] Yam JC, Zhang XJ, Zhang Y, et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children : The LAMP2 Randomized Clinical Trial . JAMA. 2023;329(6):472–481. doi:10.1001/ jama.2022.24162
[2] Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113: 2285e2291.
[3] Louis Tong, Xiao Ling Huang, Angeline LT Koh, Xiaoe Zhang, Donald TH Tan, Wei-Han Chua, Atropine for the Treatment of Childhood Myopia: Effect on Myopia Progression after Cessation of Atropine, Ophthalmology, v Volume 116, Issue 3, 200 9
[4] Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119: 347e354
[5] Chia A, Chua WH, Wen L, et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157:451e457.e1.
[6] Yam JC, Li FF, Zhang X, et al. Two-year clinical trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2020;127: 910e919
[7] Yam JC, Zhang XJ, Zhang Y, Wang YM, Tang SM, Li FF, Kam KW, Ko ST, Yip BHK, Young AL, Tham CC, Chen LJ, Pang CP. Three-Year Clinical Trial of Low-Concentration Atropine for Myopia Progression (LAMP) Study: Continued Versus Washout: Phase 3 Report. Ophthalmology. 2022 Mar;129(3):308-321. doi: 10.1016/j.ophtha.2021.10.002. Epub 2021 Oct 7. PMID: 3462780 9.
This is a case where two rare eye conditions happen to the same patient, as if they win the lottery (of the unfortunate) twice.
I saw Mary (not her real name) in her early 50s last year. She came to me because she had seen new floaters in the left eye for 1 week. I have written about floaters previously, you can find them here, here, and here for more information.
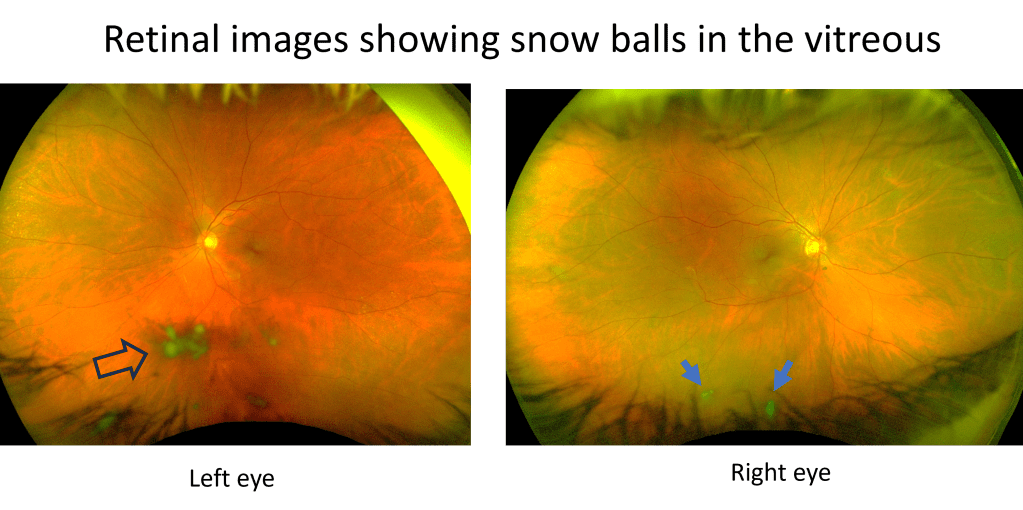
There are floaters that affect almost everyone: the regular floaters and the acute PVD (posterior vitreous detachment) floaters, and there are also weird floaters that affect only a few who win a lottery in the weird eye condition category. Mary won that lottery unfortunately. There were snow balls in her left eye, inside the jelly we call vitreous. You can see these snowballs when looking at her retina (Figure 1).
Figure 1. Initially only the left eye had intermediate uveitis, with snow balls (immune cells aggregates) in the vitreous as shown by the arrow head on the left; months later the right eye also developed intermediate uveitis with snow balls as shown by two arrows on the right.
This is called vitritis, an inflammation of the vitreous (which is the jelly inside the eyeball). When vitritis happens alone without inflammation in other parts of the eye, it is called intermediate uveitis. The most common symptom of intermediate uveitis is floaters. The snow balls are actually the immune cells accumulating inside the vitreous. It is critical we find out why inflammation happens there, because some of them can have serious health consequences to a patient’s vision and even life.
Common causes can be infections such as tuberculosis, leprosy, Lyme’s disease, syphilis, toxocariasis; autoimmune diseases such as sarcoidosis, multiple sclerosis, inflammatory bowel disease, Sjogren’s disease, tubulointerstitial nephritis and uveitis (TINU) syndrome; and cancer such as lymphoma.
I referred Mary to a uveitis specialist, who did an extensive workup and did not find a cause for her intermediate uveitis. This happens more often than not in medicine. But at least the infectious causes had been ruled out, so immune suppression treatment can be started; if the cause is an infection, then immune suppression will make things worse. She was started on oral steroids to treat the presumed autoimmune cause (though unclear what it is. She saw a rheumatologist but no diagnosis was found). She got better, but vitritis returned after the steroid taper. At that time they also found increased transaminase indicating a liver problem so no more oral steroids were given. She saw a GI specialist, who did not find a cause of increased transaminase level, and a few months later the level got better on its own.
Given the potential liver issue, no oral steroids, but eye drop steroids were given to her to treat the vitritis. She got better for sometime, but then her eye pressure spiked as a side effect of the steroid eye drops, which had to be discontinued. Meanwhile vitritis started in her right eye as well (Figure 1).
Next step of treatment would be a systemic agent that does not cause liver damage. The uveitis specialist was able to get insurance to pay for Humira (Adalimumab), and with this medication, her vitritis and floaters finally got better in both eyes up until now. This medication blocks the activity of TNF, a molecule used by our body’s immune system to create inflammation. Less TNF means less inflammation in the eyes, and it has been working for her.
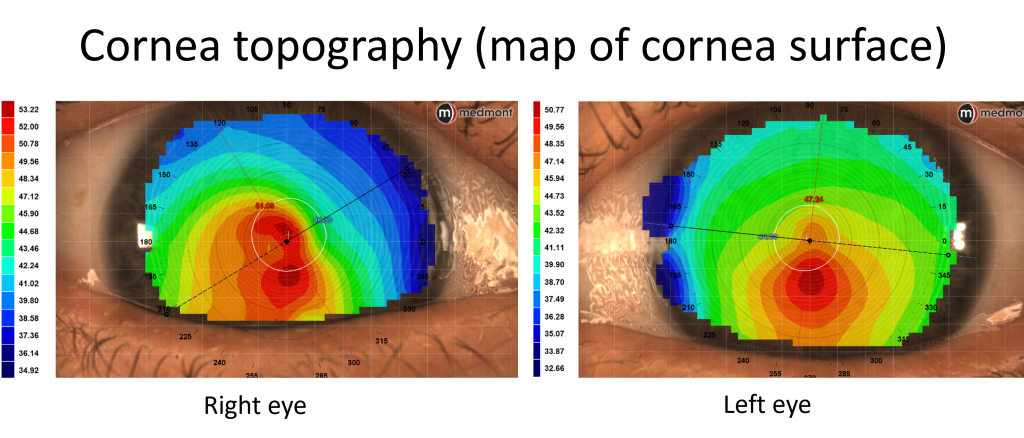
She came back to me again for new glasses now. A year ago when she first came to see me, she was wearing her new glasses of just 3 months. She had myopia and astigmatism in both eyes, more in the right eye. In that visit 1 year ago I actually found more astigmatism in the right eye and gave her an updated script. It was a little unusual to have a change in just 3 months, but she had other things to worry about for her eyes (the vitritis), so this was not pursued. Now her vision was blurry, and the right eye had a further increase in astigmatism. This is not normal. So I ordered a corneal topography, and sure enough, she actually has keratoconus in both eyes (Figure 2).
Figure 2. Surface map showing steepening of inferior cornea (evidenced by red color) in both eyes, characteristic of keratoconus.
Keratoconus is not a common eye condition, and you can read about it in my previous articles here and here. It often shows up among young people, as the disease tends to progress at a young age. For her to progress and get a diagnosis at 53, that was unusual. Talking about coincidences, I happened to have another 52 year old female patient on that same day whom I diagnosed keratoconus 6 months ago. She also started having vision problems only in the recent couple of years. Life sometimes cannot be explained by just random events, or we humans are just too good at picking up anomalies.
Anyway, the prevalence of intermediate uveitis is very low, about 6 out of 100,000 people. The prevalence of keratoconus is higher, about 5%, but still not a common condition. For her to have both, it is a chance of 3 out of 1 million. Winning two lotteries!
I would not want her luck. Getting either one of these conditions is a frustrating journey in gaining vision back. She is frequently in doctor’s offices, taking eye drops and medications probably life-long if she’s lucky enough to have the eye inflammation under control, may need eye surgeries and special contact lenses if vision continues to worsen with keratoconus.
After the new measurement of her eye powers, I gave her a new prescription. She was happy and said, ‘I haven’t had new glasses for over a year, now I’m ready to get new ones and see better.’ In fact, she sounded more positive than many of my healthy patients whose only problem was needing glasses. Happiness is a state of mind, regardless of the conditions that you may have physically.
I received a message from a patient who sounded desperate. She said that her eyeball is changing color, that she has necrotizing scleritis, and her uveitis doctor is not picking up the phone.
The last time I saw her was a year ago, she was only 22, a young and vibrant age. However her lazy eye was bothering her a lot. She had it since she was a little baby, the right eye went out with poor vision. She had patching therapy to treat lazy eye, but her vision was still 20/100 in that eye at its best.
Lazy eye is a condition that develops before 8 years of age. From birth to roughly 8 years, kids’ eyes need to receive sufficient visual stimuli to develop their visual pathway leading to normal vision. A lazy eye could be turning out or turning in, or turning up or down, which prevents this eye from getting the proper visual stimuli, leading to abnormal development of the visual part of the brain corresponding to this eye. As an adult, it becomes very difficult to treat lazy eye, as the visual brain becomes less elastic.
Not only does a lazy eye that has an eye turn affect vision in one eye permanently, it also poses a psychological and social challenge for patients. A very noticeable eye turn can cause reduced self esteem and is a problem beyond just the cosmesis. Many adults with an eye turn seek surgery to make their eyes appear straight, even if that does not change vision. When I asked if she was interested in such an option, she very happily said yes.
So I referred her to a specialist that does such surgeries for adults.
Most of these surgeries are successful, with a happy patient who feels more confident in their daily lives. Complications are uncommon.
The surgery went well for her. However, very unfortunately, a rare complication happened. Necrotizing scleritis is a rare eye condition which can be caused by autoimmune conditions. She has a preexisting autoimmune condition, psoriatic arthritis. With this condition, patients have joint pain and red scaly rashes on their skin. Her symptoms were in good control prior to the surgery. However, unfortunately the surgery and sutures triggered inflammation of the white lining of the eyeball, the sclera. Remember she has only one good eye with the other seeing poorly from being a lazy eye. Though eyes are straight, she still relies on only the good eye to see and function. The unfortunate part is that the good eye developed the necrotizing scleritis, as eye turn surgery was typically done on both eyes. Scleritis is a rare condition, necrotizing scleritis is even more rare. It is the most severe form of scleritis, with the tissue undergoing necrosis, or death. Patients have excruciating eye pain and reduced vision. The prognosis is poor, with high likelihood of vision loss.
No one could foresee such a complication to happen, but it happened. She was seeing uveitis specialists from the best eye hospital in the area, as well as rheumatologists. The silver lining of this unfortunate event is that after some time, her eye was stabilized and under control with a medication called methotrexate as well as multiple eye drops. She was doing well for some time and her vision was preserved.
Until she got pregnant. She should not get pregnant while taking the medication that she’s taking for her active autoimmune condition. It was not planned. But she’s happy with her fiance and she’s scared but loves her baby. Methotrexate is a pregnancy category X drug, which means it is not recommended to take during pregnancy. It may cause miscarriage and birth defects of the baby.
What now? She had to stop the medication. Her eye condition took a turn. It’s getting worse again, and she is being referred from one uveitis specialist to the next. She was not able to get an appointment and she told me that her eyeball is changing color. The color change in scleritis means the sclera tissue is getting thin, to the point the underlying choroid is showing through.
I am not a uveitis specialist, her case is beyond my specialty. I reached out to her specialists- I do not want to get into the details of the process- and I believe that she will be seen and treated soon.
It is not easy to be a woman. First off, women are more likely to have autoimmune conditions and more likely have severe symptoms. Well she is one of these women. Autoimmune diseases can affect young people, and she is young. Second, most medications for autoimmune conditions are not pregnancy friendly. For women at child-bearing age, if they are battling active autoimmune diseases, they hardly have a choice to have kids. If they do get pregnant, they may have to hold off the treatment and risk their conditions getting worse. There is no winning for them.
For my patient, she has bad luck to incur a rare complication after a usually very safe surgery, a surgery that she rightfully deserves. The pregnancy should have been prevented. But accidents can happen. On the one hand, she is risking losing vision in the only good eye without the medication, and on the other, she would be risking the baby if she were to resume the medication. Difficult choice and I feel very sorry that she has to choose.
UMass Chan Medical School faculty members Juan Ding, OD, PhD, and James Ledwith, MD, are working with Israeli-based AEYE Health on a pilot study testing a handheld, AI-assisted retinal camera to improve screening for diabetic retinopathy in a primary care setting.
For the pilot study, patients with diabetes seeing their physician or nurse practitioner at the UMass Memorial Health family medicine practice in Fitchburg may also be screened for retinopathy by a medical assistant or resident using an AI-assisted retinal camera. The technology is based on an algorithm developed by AEYE Health that received FDA clearance last fall. The retinal images of each eye will be quickly uploaded to an integrated cloud-based service with a corresponding report available to the physician in under a minute. The physician can then discuss the results of the screening with the patient and decide whether they need to return in one year or will need to be referred to Dr. Ding, assistant professor of ophthalmology & visual sciences, and her colleagues at the UMass Memorial Eye Center for further reevaluation.
The current screening process requires primary care physicians to refer patients to have an eye exam with an eye doctor. Dr. Ledwith, assistant professor of family medicine & community health, and Ding anticipate that the convenience of the AI camera will allow primary care practices to screen more patients.
“Only one-third of our patients consistently get their eye exam done every year and the others are going without their annual screening,” said Ledwith. “Increasing the number of patients not only requires testing in this pilot project that we’re doing, but also seeing the benefit of it in a relatively small sample of one practice and getting a camera like this into each primary care practice that’s providing care for people with diabetes.”
“Most patients know that they are supposed to have the exam done each year. Their primary care doctors and their diabetes doctors keep telling them you should go for eye exams, but they just don’t,” said Ding. “Sometimes we make an appointment, but the patient doesn’t show.”
UMass Chan and AEYE Health received an $800,000 grant for the study from the Israeli-U.S. Binational Industrial Research and Development Foundation. The study is also receiving the Herman G. Berkman Diabetes Clinical Innovation Fund grant from the UMass Diabetes Center of Excellence to help complete the pilot project after the BIRD grant expires.
The pilot study is expected to include 500 patients and launch in April.
A common condition called presbyopia happens to people older than 40 years of age. You may find it easier to read and use computers with reading glasses. Will the reading glasses weaken your eyes? Should you try NOT to use reading glasses? Find out in this short video.
This video talks about a common and very annoying eye condition- floaters. I describe my own experience with floaters and talk about risk factors of having floaters. If you suddenly see new floaters or flashes of light, don’t delay, call you eye doctor and have your eyes checked, because 15% of cases may be associated with retinal tears and detachment. Check out my previous post about floaters: https://bostoneyeblink.com/2019/11/28… One of the risk factors of having floaters early is myopia, here is the list of videos that talk about myopia prevention and control. https://www.youtube.com/playlist?list…