

By Pat Sargent February 09, 2023
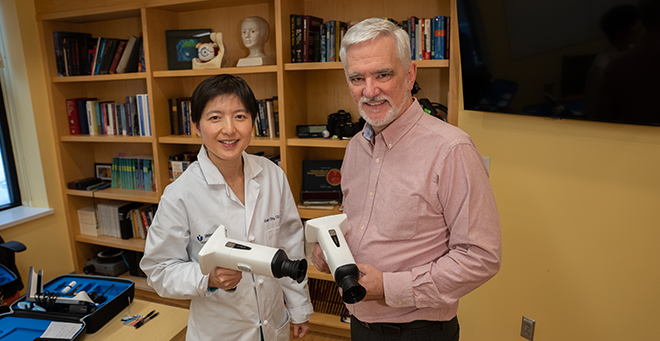
UMass Chan Medical School faculty members Juan Ding, OD, PhD, and James Ledwith, MD, are working with Israeli-based AEYE Health on a pilot study testing a handheld, AI-assisted retinal camera to improve screening for diabetic retinopathy in a primary care setting.
For the pilot study, patients with diabetes seeing their physician or nurse practitioner at the UMass Memorial Health family medicine practice in Fitchburg may also be screened for retinopathy by a medical assistant or resident using an AI-assisted retinal camera. The technology is based on an algorithm developed by AEYE Health that received FDA clearance last fall. The retinal images of each eye will be quickly uploaded to an integrated cloud-based service with a corresponding report available to the physician in under a minute. The physician can then discuss the results of the screening with the patient and decide whether they need to return in one year or will need to be referred to Dr. Ding, assistant professor of ophthalmology & visual sciences, and her colleagues at the UMass Memorial Eye Center for further reevaluation.
The current screening process requires primary care physicians to refer patients to have an eye exam with an eye doctor. Dr. Ledwith, assistant professor of family medicine & community health, and Ding anticipate that the convenience of the AI camera will allow primary care practices to screen more patients.
“Only one-third of our patients consistently get their eye exam done every year and the others are going without their annual screening,” said Ledwith. “Increasing the number of patients not only requires testing in this pilot project that we’re doing, but also seeing the benefit of it in a relatively small sample of one practice and getting a camera like this into each primary care practice that’s providing care for people with diabetes.”
“Most patients know that they are supposed to have the exam done each year. Their primary care doctors and their diabetes doctors keep telling them you should go for eye exams, but they just don’t,” said Ding. “Sometimes we make an appointment, but the patient doesn’t show.”
UMass Chan and AEYE Health received an $800,000 grant for the study from the Israeli-U.S. Binational Industrial Research and Development Foundation. The study is also receiving the Herman G. Berkman Diabetes Clinical Innovation Fund grant from the UMass Diabetes Center of Excellence to help complete the pilot project after the BIRD grant expires.
The pilot study is expected to include 500 patients and launch in April.
This video talks about a common and very annoying eye condition- floaters. I describe my own experience with floaters and talk about risk factors of having floaters. If you suddenly see new floaters or flashes of light, don’t delay, call you eye doctor and have your eyes checked, because 15% of cases may be associated with retinal tears and detachment. Check out my previous post about floaters: https://bostoneyeblink.com/2019/11/28… One of the risk factors of having floaters early is myopia, here is the list of videos that talk about myopia prevention and control. https://www.youtube.com/playlist?list…
Diabetic retinopathy remains the number 1 cause of vision loss in working-age adults in America. Key to prevent this vision loss is early screening and detection. However, the screening rate remains low world-wide as well as in the US. For many Americans, there are several barriers to accessing quality eye care which include income, distance to the nearest clinic, and health insurance among other factors. Due to these barriers, it is important to improve the methods of screening for diabetic retinopathy, as well as the adherence to recommended follow up. Recent studies have identified AI-based algorithms as promising tools for the screening and early identification of DR in at-risk individuals. Many different algorithms are being developed and the sensitivity and specificity of these algorithms needs to be evaluated before they can be clinically implemented. Further, there are limitations for the currently available AI that prevent them from being widely used clinically.
Our research aims to implement a novel AI that overcomes these limitations and improve diabetic retinal screening. We have partnered with the digital health company AEYE Health to test the diagnostic accuracy of a hand-held AI-assisted non-mydriatic funduscopic camera to be used in the primary care setting to screen at-risk individuals for retinal changes indicative of diabetic retinopathy. AEYE AI algorithm just received FDA clearance and we are in the final stage of implementing this technology in the primary care setting.
In this video, I explain what a migraine aura is, and how to differentiate it from other more sinister conditions like a stroke or retinal detachment which may cause blindness, and when you should seek medical help.
