There have been so many recent studies on this ‘novel’ treatment and I have to write about it now.
First of all, what is this treatment?
The official name is ‘repeated low level red light’. It was originally used by Chinese ophthalmologists to treat amblyopia, though there was hardly any evidence for it.
For myopia control, the red light that is used in the treatment has a wavelength of 650 nm, with 1600 lux through the pupil, and children are supposed to look at this light for 3 min x 2 per day, at least 5 days a week.
Is it a strong light? It seems so. A small number of subjects have to withdraw from these studies due to intolerance to the light. Many report after images, but most report the after images gone after 4 minutes.
If you think about it though, that is indeed a strong light. When do you ever experience after images up to even 1 minute in real life?
However, the energy that these devices emit to the retina for that treatment duration in theory is safe. Although that cannot be said to be true for all devices out in the market (see below on ‘issues and concerns’).
Does it reduce myopia progression?
A few years ago, Chinese ophthalmologists and researchers started using this device to slow myopia progression, and found it to be very effective. For example, in 2021, a multi-center, random and single blinded study recruited 264 myopic children 8-13 years of age and found that after 12 months of treatment, the red light group showed significant less myopic progression vs the control group [1].
This new therapy is attractive because it takes very little time per day to do it, perhaps just next to atropine eye drops, and it’s effective.
Any issues or concerns?
However, safety is a big concern. Indeed, there is a report about retinal damage of a child [2]. And a study shows that some of these devices actually exceed the safety limit for human retinas [3].
Another issue is that the follow up period for this treatment is usually short, about 1 year, and we don’t know if the effect is longer lasting, if the effect diminishes after longer duration of usage, or if it can be safely used for longer than 1, 2 or a few years.
Can you use it in children who are not yet myopic to prevent myopia from happening?
Further, can it be used to prevent myopia from developing in the first place? Low dose atropine seems to work [4], in addition to out door activities (so many publications on this). But will red light work too?
A study was published this month to show that the red light seems to reduce myopia incidence in premyopic children as well [5]. This study recruited premyopic children 8-13 years of age and randomly divided them into 2 groups, one control (36 children) and one receiving repeated red light therapy (40 children) 3 min x2 every day for 12 months. After 12 months, the control group showed an average of -0.52 D myopic shift and the treatment group showed -0.18 D shift. The axial length of control group was +0.29 and that of the treatment group was +0.15. The incidence of myopia was 19.4% after 12 months for the control group, and 2.5% for the treatment group. These results show a good efficacy of preventing myopia with the red light therapy. I have adapted the study data in the following figure (Figure 1).
Figure 1. Time courses of change of spherical equivalent refraction (A) and axial length (B). PM- C, premyopia- control group; PM- RL, premyopia RLRL group.
The study also included myopic children with control or red light therapy, and found that red light reduced myopia progression similar to previous studies. But I removed those lines to make it simple.
Axial length shortening
Another cool finding is that red light in some children caused a shortening of the axial length, and reduction in myopia in the first 3 months, then this effect gradually dwindled. Shortening of axial length is not commonly observed, but in certain myopia control cases, it is observed with atropine eye drops, orthokeratology lenses and peripheral defocus glasses. The red light treatment seems to have a large percentage of such shortening cases, which speaks for its good efficacy. Maximum AL shortening percentage was 53.1% in the myopic children who received red light at 3 months, and 21.9% of the subjects still had a significant shortening in AL after 12 months of treatment. In the premyopic children who received red light, maximum AL reduction was 22.5% at 3 months and 12.5% at 12- month follow- up (Figure 2).
Figure 2. The percentage of subjects showing significant AL shortening during the treatment. Axial length (AL) shortening (>0.05 mm) was defined as a significant shortening. PM- C, premyopia- control group; PM- RL, premyopia RLRL group.
Conclusion and final remarks
Recently several studies have shown that repeated low level red light therapy is effective and safe for myopia control and prevention, for the short follow up period of 12 months. Its efficacy is quite impressive, however, we wait for the longer time follow up studies of efficacy and safety.
I don’t view this as a first line treatment of myopia control or prevention, but for those unresponsive to atropine, orthokeratology, soft multifocal contact lenses and peripheral defocus glasses, this is worth trying.
What I would like to see in future studies is a dose response of this treatment. When atropine came out, carefully designed studies looked at all possible concentrations and landed us some pretty safe doses. The red light has just one intensity, one set of treatment dose and it’s used in all studies. Since the safety is the obvious elephant in the room, why not address it? Why not design studies to look at lower intensity, lower treatment duration and frequency? If there is treatment efficacy at half the intensity and even less duration and frequency, we want to know.
Another burning question is that no one knows why the red light works. Is there any intrinsic benefit of redness of the light? Or is it just intensity of the light? We all know out door activity is effective largely due to the brighter light outside. So why not design a real control group where the kids will look at another light source of 1600 lux, perhaps a white light, perhaps a green light, to find out if red light is truly sacred in myopia control? If it’s all about delivering light energy to the retina, then blue light will work even better, right? These studies will help us better understand the mechanism of this seemingly magic treatment.
References:
[1] Jiang, Y., et al., Effect of Repeated Low-Level Red-Light Therapy in Myopia Control in Children: A Multicenter Randomized Controlled Trial. Ophthalmology, 2021.
[2] Liu H, Yang Y, Guo J, et al. Retinal damage after repeated low- level red- light laser exposure. JAMA Ophthalmol 2023;141:693–5.
[3] Ostrin LA, Schill AW. Red light instruments for myopia exceed safety limits. Ophthalmic Physiol Opt. 2024; 44: 241–248. https://doi.org/10.1111/opo.13272
[4] Yam JC, Zhang XJ, Zhang Y, et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children : The LAMP2 Randomized Clinical Trial . JAMA. 2023;329(6):472–481. doi:10.1001/ jama.2022.24162
[5] Liu G, Rong H, Liu Y, et alEffectiveness of repeated low-level red light in myopia prevention and myopia controlBritish Journal of Ophthalmology Published Online First: 17 April 2024. doi: 10.1136/bjo-2023-324260
Many kids are myopic and need glasses. Sometimes the parents are worried that wearing glasses may make their eyes worse, or request to have a ‘weaker’ prescription for fear that strong prescriptions are bad for their eyes. Sometimes kids don’t wear glasses at all, despite having trouble seeing far away; mostly the kids are doing this, but I have had occasionally some parents refusing their children to wear glasses for whatever reasons.
So, when your kids have myopia, should they wear glasses?
The answer is YES. A review article [1] looking at previous research on this subject found that under-correction, which means to wear weaker glasses on purpose, more often than not, will cause the myopia to progress faster. Not wearing glasses is a form of under-correction.
When your kids have myopia, should they wear ‘weaker’ glasses?
The answer is NO. Under-correction, or wearing weaker glasses will not only make kids’ vision blurry, but also potentially make their myopia progress faster.
When your kids have myopia, should they wear glasses that are stronger than necessary?
The answer is NO. I cannot fathom why some people would want glasses to be stronger than what they should be, perhaps they want to save money when myopia progresses so that they don’t need to buy another pair? In any rate, it’s not good practice either, as stronger prescription does not help and may actually cause myopia to progress faster as well.
So there you have it, for children with myopia, a proper prescription of glasses is necessary, not weaker, not stronger, but just right. This way they will see well and myopia progression is not worsened by not having glasses or having the wrong glasses.
Reference
[1] Logan NS, Wolffsohn JS. Role of un-correction, under-correction and over-correction of myopia as a strategy for slowing myopic progression. Clin Exp Optom. 2020 Mar;103(2):133-137. doi: 10.1111/cxo.12978. Epub 2019 Dec 18. PMID: 31854025.
[1]Yam JC, Zhang XJ, Zhang Y, et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children: The LAMP2 Randomized Clinical Trial. JAMA. 2023;329(6):472–481. doi:10.1001/jama.2022.24162
[2]Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113: 2285e2291.
[3]Louis Tong, Xiao Ling Huang, Angeline L.T. Koh, Xiaoe Zhang, Donald T.H. Tan, Wei-Han Chua, Atropine for the Treatment of Childhood Myopia: Effect on Myopia Progression after Cessation of Atropine, Ophthalmology,vVolume 116, Issue 3, 2009
[4]Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119:347e354
[5]Chia A, Chua WH, Wen L, et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157:451e457.e1.
[6]Yam JC, Li FF, Zhang X, et al. Two-year clinical trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2020;127: 910e919
[7]Yam JC, Zhang XJ, Zhang Y, Wang YM, Tang SM, Li FF, Kam KW, Ko ST, Yip BHK, Young AL, Tham CC, Chen LJ, Pang CP. Three-Year Clinical Trial of Low-Concentration Atropine for Myopia Progression (LAMP) Study: Continued Versus Washout: Phase 3 Report. Ophthalmology. 2022 Mar;129(3):308-321. doi: 10.1016/j.ophtha.2021.10.002. Epub 2021 Oct 7. PMID: 34627809.
[8]Wang W, Zhang F, Yu S, Ma N, Huang C, Wang M, Wei L, Zhang J, Fu A. Prevention of myopia shift and myopia onset using 0.01% atropine in premyopic children – a prospective, randomized, double-masked, and crossover trial. Eur J Pediatr. 2023 Jun;182(6):2597-2606. doi: 10.1007/s00431-023-04921-5. Epub 2023 Mar 22. PMID: 36944782.
We all know that the sunlight is the best light to prevent and control myopia in children. I have previously published multiple media items to talk about this and you can view them here. Indeed playing outside is the best way to prevent myopia. However, given the modern lifestyle, it is inevitable that we are still spending majority of the awake time inside a house, be it home, school, work or even entertainment. What can we do to reduce myopia while inside the house?
The key is to ensure that children have sufficient ambient light when staying indoors [1,2], including doing all activities, such as studying, eating, having fun, that is, except for sleeping at night.
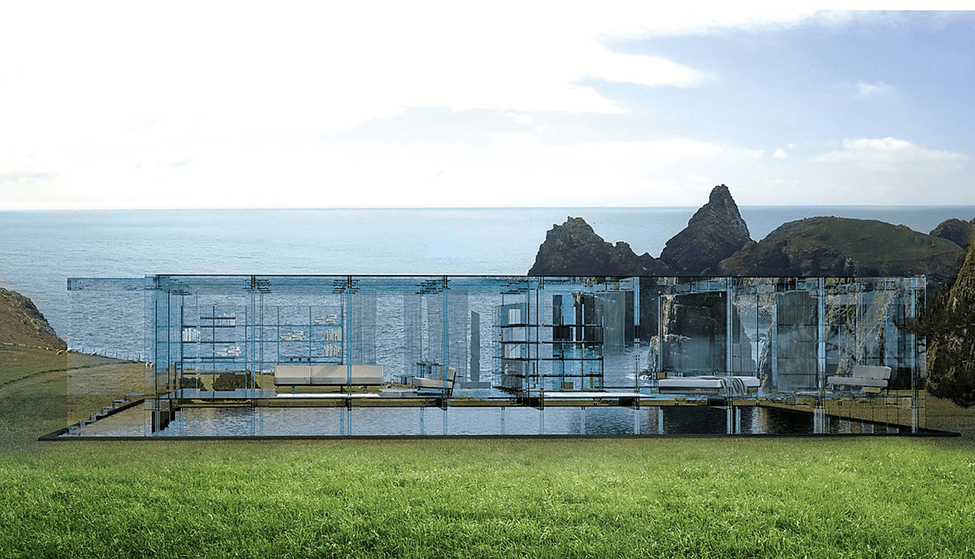
If you can afford a glass house such as the one below, then you are all set. The sun will be your light source. It’s like you are living outside all the time. No one will develop myopia in such a house, ever.
However, as dreamy as this house may be, you and I most likely will never get to live in one, so we have to resort to having good lamps.
Living in New England, most of the houses here are old, without the floor to ceiling windows you see in modern homes, and winter here is basically 6 months long with extended dark nights. Mind you, it gets dark at 4 PM, so when you get home from work or school, you will not have any natural light to do myopia-preventing outdoor activities. This will be a good time to crack up your home light intensity. The brightest light indoors is still several orders of magnitude weaker than outdoor sunlight. So never worry that your light may be too bright. On the contrary, always worry that your light is too dim.
Most homes will use some or all of the lighting sources: desklamp, floor lamp or ceiling lamp. I will provide some guidelines for how to choose a good one for myopia control for each of these.
Desk lamp
1. Sufficient brightness
Desk lamps should provide sufficient brightness to ensure that reading materials such as books, documents, and screens are clearly visible and reduce eyestrain. Usually, the suitable reading brightness is about 300 to 600 lumens.
2. Good color accuracy
Choose desk lamps with a high color rendering index (high Ra) as they can render colors more accurately and reduce visual fatigue. By definition, Ra under natural light is set as 100. When you choose a desk lamp, try to choose Ra95 or above, so that the color accuracy is closer to that under natural light.
3. Good uniformity of illumination
Make sure the light from the desk lamp is evenly distributed and does not create noticeable shadows or glare. The smaller the variation in lighting, the less likely it is that the pupils will dilate or constrict, which can lead to visual fatigue.
4. Comfortable color temperature [3, 4]
The color temperature of a light is an indicator that describes its color appearance, usually expressed in units of Kelvin (K). Different color temperatures will produce different visual effects. Here are some differences between different color temperatures:
Lower color temperatures (2700K – 3000K): Lower color temperatures typically appear as warmer tones, similar to yellow or orange light. This color temperature is warm and comfortable, suitable for casual environments.
Medium color temperature (3500K – 4500K): Medium color temperature usually appears as natural white or natural daylight color. This color temperature is fresh and neutral, which is more suitable for studying. It helps improve alertness and concentration.
Higher color temperature (above 5000K): Higher color temperature appears as cool colors, similar to a bluish white light. This color temperature is typically used in environments that require a high degree of lighting and visual precision, such as operating rooms, laboratories and workshops. Higher color temperatures can increase alertness and concentration, but may feel cold when used in a home environment.
In addition, the color temperature of the lights can also be adjusted between different activities and time periods to suit different needs.
For example, you can use a medium color temperature when studying during the day; and at night, if you plan to read a book before going to bed, you can adjust the color temperature to a lower color temperature to help you relax and get ready for asleep.
Some desk lamps can have settings to adjust between different color temperatures as well as brightness of the light, which are helpful.
5. Ability to adjust brightness
Even though it is beneficial to prevent myopia by using as bright a light as possible, in some cases, you may find it difficult to tolerate bright light, such as when you have dry eye syndrome, conjunctivitis, or migraine headaches. Turn down the brightness if you suffer from these conditions.
6. Blue light
There is a lot of debate about blue light for eye health. Blue light is part of the natural visible light spectrum. A normal dose of blue light exposure is good for the eyes, circadian rhythm, and a happy mood, but excessive exposure is bad [5].
The visible light spectrum of sunlight is a continuous spectrum, including blue light and all the way to red light. Compared with natural light, the spectrum of many LED lights contains a disproportionately high amount of blue light. When you choose desk lamps, try to choose light bulbs with a continuous spectrum and no excessive blue light.
7. Avoid flickering
Desk lamps should not produce significant flicker, as flickering light sources may cause eye discomfort.
8. Proper positioning, height and angle
Place the desk lamp in a suitable position to ensure that the reading material is illuminated without the light shining directly into the eyes. Avoid light shining on the screen or reflect onto your eyes. Some desk lamps have adjustable arms, lampshades, diffusers or beam angles that allow you to adjust the direction and range of light as needed.
9. Additional functionality
Some modern desk lamps come with remote controls, touch controls, or smartphone app controls for easier operation and adjustment. These have nothing to do with myopia control and can be selected according to personal preferences.
10. Energy efficiency
Choosing energy-efficient desk lamps can reduce energy consumption, help save money on electricity bills, and be greener on the environment. LED desk lamps generally have high energy efficiency. Although our focus is on preventing myopia, it would be better if it could also save energy.
Although desk lamps are the direct source of light for children to study, the lighting of the environment in which children live and play is also important. When we are outdoors, the entire environment is bright, not just the 40 centimeters in front of our eyes.
So while using a desk lamp, you can also consider turning on a floor lamp or ceiling lamp. The considerations for selecting these lamps are similar to those introduced before for desk lamps, but there are a few additional considerations.
∎For ceiling lights, good design and shading should also be considered: tryto prevent the light from directly entering the eyes.
∎For floor lamps, in addition to good design and shading, you can also consider the appropriate height and whether the light direction can be adjusted: Some floor lamps have adjustable arms or lampshades, allowing you to control the direction and range of light.
Good indoor lighting is necessary not only in the study room, but the entire environment should be as bright as possible. For example, install a good ceiling light above the dining table so that family can enjoy food in a nice a bright environment. If you are like me, you would spend a good amount of time eating dinner every day. Many families have a sunroom for children to play in, which is a fantastic idea. If children are playing or watching TV in the living room, it will be beneficial to add ceiling lights or additional floor lamps to increase the brightness of the environment.
In summary, the best indoor lighting for myopia control is bright illumination as well as a few other perks, possibly utilizing multiple light sources throughout the house. Ideally this is in addition to the out door activities, not instead of them.
References:
[1] Jiang X, Kurihara T, Torii H, Tsubota K. Progress and Control of Myopia by Light Environments. Eye Contact Lens. 2018 Sep;44(5):273-278. doi: 10.1097/ICL.0000000000000548. PMID: 30048342
[2] Landis EG, Yang V, Brown DM, Pardue MT, Read SA. Dim Light Exposure and Myopia in Children. Invest Ophthalmol Vis Sci. 2018 Oct 1;59(12):4804-4811. doi: 10.1167/iovs.18-24415. PMID: 30347074
[3]Weitbrecht WU, Bärwolff H, Lischke A, Jünger S. Wirkung der Farbtemperatur des Lichts auf Konzentration und Kreativität [Effect of Light Color Temperature on Human Concentration and Creativity]. Fortschr Neurol Psychiatr. 2015 Jun;83(6):344-8. German. doi: 10.1055/s-0035-1553051. Epub 2015 Jun 22. PMID: 26098084.
[4]Chao Wang, Fan Zhang, Julian Wang, James K. Doyle, Peter A. Hancock, Cheuk Ming Mak, Shichao Liu, How indoor environmental quality affects occupants’ cognitive functions: A systematic review, Building and Environment, Volume 193,2021,107647,ISSN 0360-1323,https://doi.org/10.1016/j.buildenv.2021.107647.
[5]Wahl S, Engelhardt M, Schaupp P, Lappe C, Ivanov IV. The inner clock-Blue light sets the human rhythm. J Biophotonics. 2019 Dec;12(12):e201900102. doi: 10.1002/jbio.201900102. Epub 2019 Sep 2. PMID: 31433569; PMCID: PMC7065627.
Yes, low dose atropine can lower myopia risk if used in children without myopia in this Hong Kong study. However, even without it, 47% of the studied children did not develop myopia after 2 years. In those using 0.01% atropine, 54% did not develop myopia, and in those using 0.05% atropine, 72% did not develop myopia. A dose dependent effect of myopia prevention can be inferred. But whether to use atropine or what dose to use should be an individualized process.
This article is also available in an audio podcast format in case you want to give your eyes a break. Click here to listen.
Official full text below
Recently, the University of Hong Kong published a paper [1] to study whether two different concentrations of low-dose atropine can prevent the development of myopia for children whose eyes are not yet myopic. This is a randomized double-blind study involving more than 400 children aged 4-9 years old with 0-1.00 diopters of hyperopia. About 1/3 received placebo, 1/3 used 0.05 % atropine once daily, and 1/3 used 0.01 % atropine eye drops once daily for two years, and the development of myopia was observed in these children. The study found no statistically significant difference using atropine 0.01% compared with placebo. In contrast, atropine at a concentration of 0.05% was able to delay the progression of myopia. After this article came out, many people had doubts. Wasn’t it shown that atropine at a concentration of 0.01% can control the growth of myopia? Why can’t it play a role in preventing myopia? So should we not use 0.01% atropine at all, but should use 0.05% instead?
To explore this issue, we need to understand the history of atropine used to control myopia.
It was discovered decades ago that 1 % atropine (note the high concentration) could slow down the progression of myopia. However, relatively high-quality evidence, such as a randomized, double-blind clinical study, was not published until 2006. In 2006, a clinical study conducted in Singapore confirmed that 1 % atropine was used for 2 years to effectively control myopia, reducing myopia by 7 7% [2]. Of course, its side effects are also very significant. 1% atropine is a common drug used to dilate pupils for fundus examination or for cycloplegic refraction. It can effectively dilate the pupils and completely paralyze the ciliary muscle of the eyes, so the eyes will be very light sensitive and blurry when looking at near objects. This side effect makes it unrealistic to use 1% atropine to control myopia. Almost no one can tolerate such side effects, especially considering that myopia control is done over many years, due to myopia progression naturally stops only between the ages of 16 and 18. Another disadvantage of 1% atropine for myopia control is that myopia progression actually rebounded remarkedly after discontinuation [3].
Later, scholars in Singapore did more randomized double-blind studies [4], they studied whether lower concentrations of atropine besides 1% atropine can also play a role in controlling myopia, which may have less severe side effects. They studied concentrations at 0.5%, 0.1%, and 0.01%. In this study, scholars found that the effect of atropine on controlling myopia is a concentration-related. That is to say, the higher the concentration, the better the effect of controlling myopia. But the side effects are also dose dependent. Another result that surprised them is that 0.01%, which is equivalent to diluting 1 % atropine 100 times, can still play a role in controlling myopia. And this concentration of atropine has almost no mydriatic (pupil dilating) effect and side effects. This study was also observed for two years.
At the third year, all children stopped using atropine, and the researchers wanted to see whether myopia would continue to grow. They found that after stopping the relatively high concentrations of atropine (0.5 % and 0.1 %), the myopia rebounded, that is to say, the speed of myopia progression increased faster than average myopic children. But surprisingly the 0.01% concentration of atropine showed no such phenomenon of rebound [5].
The study found that the side effects of atropine at a concentration of 0.01% are very low. Although there are some side effects of mydriasis and loss of accommodation, the vast majority of children are not disturbed, and they can still see normally.
This result suggests that although the concentration of 0.01% atropine is very low, it can effectively control myopia, and the side effects are also the lowest. It is conceivable that the safety is also the best. After this research was published, many countries in Asia began to use 0.01% atropine to control myopia in children. At the same time, people started to steer away from the relatively high concentration of atropine (a concentration greater than 0.1 %), because these high concentrations may not only have worse side effects, but also rebound after discontinuation.
However, at this time, there is no research on concentrations in between 0.1% and 0.01%. Will they also be effective in controlling myopia? How about the side effects? What about myopia rebound after discontinuation?
To answer these questions, researchers at the University of Hong Kong conducted research on this issue. They recruited children who had already developed myopia and randomly assigned them to placebo, 0.01%, 0.025%, and 0.05% concentrations of atropine once a day. Their research also found that the effect of atropine on controlling myopia has a dose dependent effect, and the higher the concentration, the better the effect of controlling myopia. The effect of atropine 0.025% and 0.05% in controlling myopia is better than that of 0.01% [6]. Reenforcing previous research, compared with placebo, atropine at a concentration of 0.01% can still control myopia. The researchers also tested the children’s accommodation and how pupil size was affected by these different concentrations of atropine. It turns out that it is also related to the concentration, that is to say, the higher the concentration, the greater the side effects. However, even atropine at a concentration of 0.05% is still tolerated by most children.
After the two-year study, they also stopped using the drug for a year to see if the myopia would rebound. This result is also related to the concentration of atropine. If the concentration is slightly higher, such as 0.05%, the rebound will be slightly more. Of course, this rebound is much smaller than the rebound of atropine with a higher concentration such as 0.1%, 0.5% and 1%. The lowest rebound is still 0.01% [7].
These results are actually quite consistent with the previous results in Singapore. Generally speaking, we know that the higher the concentration of atropine, the better the effect of controlling myopia, but even at a concentration of 0.01%, it is already effective. In terms of side effects, atropine at a concentration of 0.05% or lower are relatively easy to tolerate, and more than this concentration will be worse, and more children will not be able to tolerate it. Therefore, it is generally believed that atropine with a concentration of 0.05% or lower should used, and atropine with a higher concentration is not recommended. In particular, there are other means to control myopia, such as orthokeratology lenses, peripheral defocused spectacles, and soft multifocal contact lenses, so it is not necessary to insist on a high-concentration atropine, which will reduce quality of life. Since the long-term safety of atropine is still under study, it is important to minimize drug exposure, using a relatively low concentration and with the shortest duration possible. The rebound phenomenon after discontinuation also needs attention, as there may be many children who will not be able to use atropine all the years until they are 18. From this point of view, 0.01% concentration of atropine is still a good choice.
These previous studies were conducted on children who had already developed myopia. But more and more parents are asking, since low-concentration atropine can effectively control the growth of myopia, can I use it when my child is not yet myopic, so as to prevent my child from developing myopia, maybe he will never develop myopia?
The current study by the University of Hong Kong helped us answer this question. The data of this study tell us that the use of 0.01% and 0.05% atropine to prevent the development of myopia is relatively safe, and the side effects in these children are also relatively low, and most children can tolerate it. The effect of 0.05% concentration of atropine is significant. But they also found that 0.01% atropine was not much different vs controls. So should 0.01% concentration of atropine be abandoned?
We have to analyze this issue with logic. Though this new study unfortunately did not include the 0.02% concentration, a trend can be seen from the data that the effect on the prevention of myopia is dose dependent. Atropine at a concentration of 0.01% was actually better than placebo (Figure 1), though this result did not reach statistical significance. Myopia developed in 45.9% of the children given atropine 0.01% compared with 53% of the children given the placebo.
Figure 1. Myopia prevention by atropine. In the beginning, none of the children had myopic (the value was 0). As time went by, more and more children developed myopia. But the children who received 0.05% atropine had the lowest rate of myopia. The blue line is the placebo group, the black line is the 0.01 % atropine group, and the orange line is the 0.05 % atropine group. The chart comes from reference [1]
I think the results of this study are quite consistent with previous studies on myopic children, that is to say, the higher the concentration, the better the effect of atropine on controlling or preventing myopia. This is straightforward, logical, and supported by a lot of previous data. So the 0.01% is just a dose that is very low, that in certain population the effect is not significant enough. And this population happens to be one that even without any intervention, myopia does not develop in half the children, as shown by the placebo group. That is to say, even in the group of children who received atropine at a concentration of 0.05%, perhaps half of the children did not need to use it at all and would not develop myopia.
On the other hand, though 0.05% atropine is effective, it is not 100% effective. After two years of intervention, approximately 28.4% of children in the 0.05% atropine group were still myopic. So it is clear that 0.05% atropine can indeed reduce the risk of developing myopia within two years, but it cannot completely avoid the occurrence of myopia.
This is the conclusion of the research. There is naturally a big difference between real life and research. In the study, a child is randomly assigned to a treatment regimen for a time set by the study, say in this case two years. In real life, of course, it is impossible to apply a fixed method to a child, regardless of the effect of the method itself over years. For example, in real life, we may give a child 0.01% concentration of atropine to control myopia. If it is observed that the control effect is not very good, we will switch to other methods, such as increasing the concentration of atropine, or changing to orthokeratology lenses or soft multifocal contact lenses, instead of continuing to use the same method mechanically. Therefore, the enlightenment brought to us by a study is mainly the effect and safety of the treatment method itself. Based on this information, we can apply the methodology to treat patients. It is not an automatic copying of the research.
What we know so far is that the safety of low-concentration atropine between 0.01% and 0.05% is relatively good, and most children can tolerate the side effects. In children who are already myopic, it can control myopia, and the higher the concentration within this range, the better the control effect. We also know now that even in non-myopic children using these concentrations of atropine can reduce the risk of myopia development, a similar dose dependent effect can be inferred. But this does not mean that when children are not nearsighted, 0.05% concentration of atropine should be used to prevent myopia automatically. Consider that 47 % of children do not develop myopia within two years even without any medical intervention. If 0.05% concentration of atropine is blindly given to every child, this will increase unnecessary drug exposure to nearly half of the children.
For those children whose parents are myopic, and whose eye axial growth is relatively fast and hyperopia is declining rapidly, if the parents and children have a strong motivation to prevent the development of myopia, 0.05% can be considered in this scenario. But for a child with relatively stable hyperopia and normal eye axial growth, it is not necessary. It is safer to observe regularly and intervene only after changes are detected.
Even after children develop myopia, what kind of concentration to use is a personalized treatment process. Atropine at a concentration of 0.01% can indeed reduce the rate of myopia increase, which has been confirmed in many clinical trials. A more reasonable consideration is to use 0.01% concentration of atropine to control after the development of myopia, and observe regularly for six months to one year. If the effect is not good, then increase the concentration to 0.05% , add/or use other controls model. Because there are indeed many children who can get effective myopia control after using 0.01% concentration of atropine alone, with the least rebound effect and side effects. If you use a relatively high concentration directly without trying a low concentration first, you will not know whether the child can effectively control myopia with only a lower concentration, which is not conducive to reducing drug exposure.
As a parent, you can communicate with the doctor to formulate a personalized treatment plan that suits your child, instead of blindly following the trend and using atropine with a relatively high concentration for control.
To summarize the existing research results of atropine in controlling myopia: atropine can effectively control the growth of myopia, and this effect is related to the concentration, the higher the concentration, the better the effect. However, the higher the concentration, the greater the side effects, and the more rebound after discontinuation. At present, it is found that 0.01%, and 0.025% and 0.05% concentrations of atropine can effectively control the further growth of myopia. And their side effects are acceptable to most children. For prevention of myopia, 0.05% concentration of atropine can also be considered. Atropine at a concentration of 0.01% has no significant difference from placebo in the prevention of myopia in one study so far. But the current study is limited to children in Hong Kong, and the follow-up is only two years. In fact, for an individual child, what method to use to prevent or control myopia should be a personalized plan for the child and their family.
References
[1] Yam JC, Zhang XJ, Zhang Y, et al. Effect of Low-Concentration Atropine Eyedrops vs Placebo on Myopia Incidence in Children : The LAMP2 Randomized Clinical Trial . JAMA. 2023;329(6):472–481. doi:10.1001/ jama.2022.24162
[2] Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113: 2285e2291.
[3] Louis Tong, Xiao Ling Huang, Angeline LT Koh, Xiaoe Zhang, Donald TH Tan, Wei-Han Chua, Atropine for the Treatment of Childhood Myopia: Effect on Myopia Progression after Cessation of Atropine, Ophthalmology, v Volume 116, Issue 3, 200 9
[4] Chia A, Chua WH, Cheung YB, et al. Atropine for the treatment of childhood myopia: safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology. 2012;119: 347e354
[5] Chia A, Chua WH, Wen L, et al. Atropine for the treatment of childhood myopia: changes after stopping atropine 0.01%, 0.1% and 0.5%. Am J Ophthalmol. 2014;157:451e457.e1.
[6] Yam JC, Li FF, Zhang X, et al. Two-year clinical trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology. 2020;127: 910e919
[7] Yam JC, Zhang XJ, Zhang Y, Wang YM, Tang SM, Li FF, Kam KW, Ko ST, Yip BHK, Young AL, Tham CC, Chen LJ, Pang CP. Three-Year Clinical Trial of Low-Concentration Atropine for Myopia Progression (LAMP) Study: Continued Versus Washout: Phase 3 Report. Ophthalmology. 2022 Mar;129(3):308-321. doi: 10.1016/j.ophtha.2021.10.002. Epub 2021 Oct 7. PMID: 3462780 9.
This article is for eye doctors who use axial length routinely in their myopia control clinic, and certain parents who are curious and/or obsessed with the numbers of their children’s eyes (trust me, I do encounter these parents weekly).
Briefly, axial length is the length of the eyeball, which grows throughout the first 18 years of a person’s life. It is normal for the eyes to grow longer over time until it stabilizes at adulthood. But the growth can be accelerated resulting in long axial length in myopia. Therefore in many eye doctors’ offices, this value is measured to monitor myopia development and record whether myopia control is successful with a given intervention.
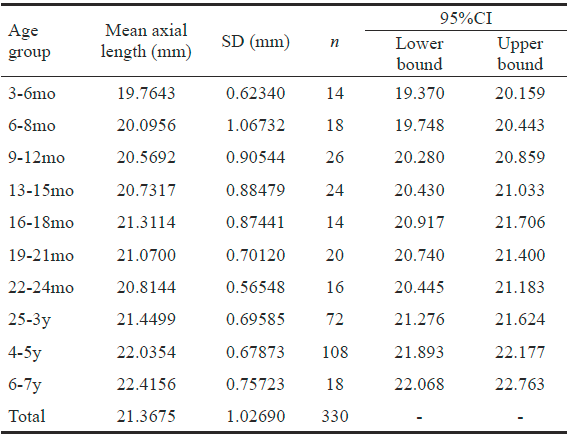
Understandably, it is important to have a normative database to evaluate whether a given child’s axial length is normal. Basically, there have been quite a few published articles on typical axial lengths of children of various ages. I have put together data from two recent studies that encompass ages from 3 months to 18 years below. The mean values for a given age are listed, as well as standard deviation. Table 1 is from Florida, USA, on 165 American children (Miami study) [1] and table 2 is from Shanghai, China, on 14,127 Chinese children (Shanghai study) [2]. Obviously the 2nd study is a much larger scale, and I really am very excited about this very new data. The first study, though with much fewer subjects, is quite remarkable as well in my opinion, as it examined kids as early as 3 months, understandably not easy to do and not many other studies were able to look at this age group. So I am keeping these two tables as a reference for my own patients.
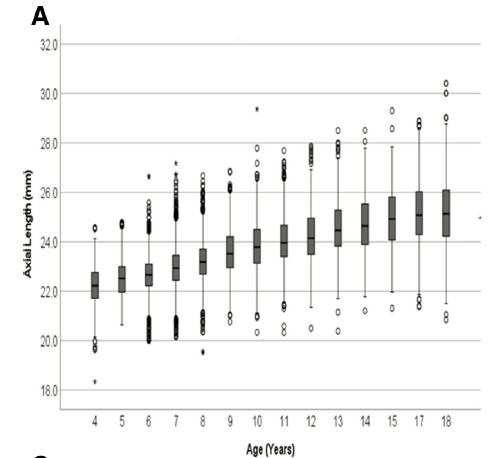
For those who are more visual, Figure 1 and Figure 2 are these numbers plotted in graphs.
Table 1. Axial length of 3 month to 7 years old children (Miami study)
Table 2. Axial length of 4 to 18 years old children (Shanghai study)
Figure 1. Axial length mean (solid line) and 95% confidence interval (dotted lines) in 3 month to 7 years old children (Miami study).
Figure 2. Axial length ranges in 4 to 18 years old children (Shanghai study).
A few things to keep in mind from these data.
First, these are from two distinct populations. The 3 month to 7 years old study group (Miami study) were children from Miami, FL. No ethnic background information was given in the paper, but one can assume it could be typical from that area. The 4 to 18 years old study group (2nd Shanghai study) were Chinese children. It is well known that Chinese children have longer axial lengths than Caucasions and African descents (and more prevalent myopia rates unfortunately), so we certainly cannot assume that this is inclusive of all possible scenarios.
Second, you can see that for any given age, there is a wide range of axial lengths in both studies. This tells us that normal is a range, NOT a single number. Do NOT compare the number of your child to your neighbor’s kids. This is not a competition. Also, it has been demonstrated again and again that it is the rate of axial length growth, rather than the absolute number, that better predicts myopia progression. Do not get anxious over one measurement. Monitor the axial length over time to find the trend.
Lastly, I would still stress that while it is great that we have a normative database for axial length, it is still the gold standard to perform cycloplegic refraction to accurately assess a child’s true refractive error. Axial length measurement is a powerful tool, but it does not and cannot replace cycloplegic refraction.
References:
[1] Miami study: Bach A, Villegas VM, Gold AS, Shi W, Murray TG. Axial length development in children. Int J Ophthalmol. 2019;12(5):815-819. Published 2019 May 18. doi:10.18240/ijo.2019.05.18
[2] Shanghai study: He X, Sankaridurg P, Naduvilath T, Wang J, Xiong S, Weng R, Du L, Chen J, Zou H, Xu X. Normative data and percentile curves for axial length and axial length/corneal curvature in Chinese children and adolescents aged 4-18 years. Br J Ophthalmol. 2021 Sep 16:bjophthalmol-2021-319431. doi: 10.1136/bjophthalmol-2021-319431. Epub ahead of print. PMID: 34531198.
We know that ortho K lenses and low dose atropine (0.01%) both can slow down the rate of myopia progression by about 50%. People often wonder whether by combining the two, we can slow down the progression even further.
Here is an article looking at a combo of the two in 73 Chinese children who have very fast myopia progression. They discovered that additional atropine 0.01% did not result in significant difference compared with ortho K lens alone in terms of axial growth.
This is disappointing. However, this study looked at children with fast myopia progression despite using ortho K lenses. Also only a small number of children were evaluated. In addition, this is a retrospective study, meaning authors looked at the data later, rather than a randomized controlled study, so there could be factors stewing the results.
Anyway, we await more studies to see whether the two have synergistic effect.
Reference:
Chen Z, Zhou J, Xue F, et al, Two-year add-on effect of using low concentration atropine in poor responders of orthokeratology in myopic children British Journal of Ophthalmology Published Online First: 11 March 2021. doi: 10.1136/bjophthalmol-2020-317980
Covid-19 has really affected so many aspects of our lives. With all that isolation inside, and the remote learning with digital screens, parents worry about their kids’ health. Many worry this will do great havoc to their eyesight, and they are not wrong.
Research has shown that confinement to home due to covid-19 is associated with an increase in myopia. Scientists have been monitoring the refractive error of 123 535 Chinese children since 2015. While the refractive error was showing a pretty steady trend in kids 6 to 8 years of age from 2015 to 2019, there was a sharp and dramatic change toward myopia in 2020 (Figure 1). Many Chinese children already don’t get enough outdoor activities and spend way too much time studying, and the covid-19 put extra strain in terms of even further decrease of outdoor time and increase of screen time.
Figure 1. Young children show a dramatic increase in myopia in 2020 compared to previous years [1]. Figure from reference [1]
I only hope that with universal vaccination and a good hygiene habit that we have formed during the past year, children will be able to be back to school and enjoy normal outside activities soon. If you think you child may have trouble seeing, please bring them to an eye doctor.
[1] Wang J, Li Y, Musch DC, et al. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement. JAMA Ophthalmol. 2021;139(3):293–300. doi:10.1001/jamaophthalmol.2020.6239
A friend who is a rehabilitation therapist in China told me some interesting observation he has had while treating myopic children. He noticed that for those children who are more anxious, their myopia progressed faster, versus those who are calmer. So he asked me whether anxiety and other psychological factors may contribute to myopia development and progression.
Now I know that when I was 10 and started becoming myopic, I had a lot of anxiety and depression, for the reason that I could not see the blackboard in class! Every school year we went to the hospital to have physical exam and the vision exam was the most anxiety-inducing. I would squint, guess, and peek at the tumbling E beforehand trying to memorize them. My face became red and my hands sweaty. Yes I am ashamed to admit that I cheated in the vision screening in elementary school to get away with a failed report to the teacher and my parents. Why did I do that? As a child I could not describe it exactly. But I did not want to wear glasses and became different from everyone else. Plus, as a straight A student, a failed test in any form was not acceptable.
More and more I found it difficult to see the board. I would nonchalantly walk up to the board then back to my seat (fortunately I sat in the middle so did not have to walk too long to disturb the other students). I would peek at my desk mate’s notes to see what’s going on. I became afraid of math classes because the numbers were small. Eventually I had to tell my parents that I had trouble seeing the board. I remember feeling ashamed when I had to tell them. It’s as though I contracted a disease that I should not have. Though the science at the time was not clear, at least to me, I knew that I was to blame for becoming near-sighted. I was always reading, day and night. Not necessarily school-related, but I was hooked by fictions, story books, magazines and newspapers, anything that had prints on them. Outside classroom, I would read on my own. During summer and winter vacation, I would still be reading books from the library. My dad who’s a teacher and scholar, was the role model that I took after. He did not stop my prolonged near work. My childhood home was very dark, with rather dim lighting. Plus my dad also had myopia though my mom had hyperopia. Thus odds were really against me and no surprise I was among the early ones in my class to wear glasses. That was in the early 1990s, at age 10 I developed myopia while majority of my classmates were still emmetropic. Today probably majority of kids in a 4th grade classroom are wearing glasses. Times have really changed.
I remember going to the hospital to have my eyes examined. The doctor put eye drops in my eyes, I had to wait for a long time, before someone put a strange-looking frame on my face and showed me a bunch of different lenses. I was asked to read letters on a chart, and I felt strange that I was able to see some tiny letters. I had to say that this cycloplegic trial frame refraction was up to American standard even to this day. Thanks to my small town ophthalmologist, I was finally able to see. I was -2.00 in both eyes that day and I no longer had to walk up to the board to see small prints.
Back to our question on myopia and anxiety. My own experience told me that as a myope without glasses, I definitely felt anxiety. After wearing glasses, my vision was back, but I felt a kind of depression because I had to rely on glasses and I hated having to glasses. I went through all 5 stages of grief: denial, anger, bargaining, depression and acceptance. I thought that if I looked far away long enough, my eyes would be back to normal. I was mad at myself for abusing my eyes without a break on those stupid books. I constantly regret it and promised I would trade in some years of my life in exchange for normal eyesight. I was depressed that I had to wear glasses and looked ugly. Eventually of course I accepted this imperfect aspect of me. After all, there were so many other things that were not perfect so why focus only on myopia?
As an optometrist, myopia is one of the most common conditions we treat. It’s so common we almost consider it ‘normal’, routine and benign. We rarely considered the psychological aspect of myopia, when in reality this condition hit children and adolescents, who are at a vulnerable age.
Now the science part of this article. Research has shown that myopic teenagers had more anxiety than their peers, and boys with myopia had more anxiety than girls with the same condition 1. However, personality profile and psychophysical stress do not seem to play a primary pathogenetic role in myopia 2. So that is good, you can feel tortured by the fact that you need thicker glasses, but the sadness alone does not make your eyesight worse.
Myopia has become a global epidemic, affecting kids of school age, sometimes as early as 6 or 7. Left untreated, myopia may progress 1 diopter each year, resulting in high myopia when kids become adults. Myopia is not just an inconvenience, it is an eye disease that significantly increases a person’s risk of developing retinal detachment and myopic macular degeneration, both can lead to blindness.
Naturally parents become concerned when their kids fail the vision screening at school and have to wear glasses to see well. As food is a key part of our health, many often wonder if food contributes to myopia development. For example, does eating sugar and refined carbohydrates increase myopia? Surely sugar is bad for your teeth and just bad for your health in general. Is it also to blame for myopia?
Will sugar coma cause you to see worse?
When I was a student at New England College of Optometry in Boston, we learned extensively on myopia, which is a major topic of interest for optometry. While many factors affect myopia, for example, genetics, prolonged near work, lack of outdoor activities, sugar intake was never mentioned as a factor to affect myopia. Yes diabetes can affect a person’s vision by making them temporarily more myopic or hyperopic, but that is reversible and after blood sugar levels are controlled, the eye returns to baseline refractive state. Most people, especially school aged children, do not have diabetes or constantly fluctuating sugar levels. So is there any evidence for a role of sugar in myopia that is not in context of diabetes?
It turns out not many studies have been done on this topic. In 1956, Gardiner proposed that carbohydrates and fats in the diet could cause myopia 1, but this hypothesis was discarded later in the scientific community. When this happens, it’s either because not enough research was done to support it, or that it did not hold water by subsequent research. In deed there was a scarce of literature on this topic. But one actually found that more sugar intake did not increase risk of developing myopia in children 2. This study in turn, found out that too much saturated fatty acid in the diet correlated with more myopia.
Most recently a French study evaluated 180 children aged 4-18 via questionnaire about their diet habits, and discovered that for girls, more sugar and refined carbohydrates correlated with more myopia, but in boys, this was actually the opposite, that is, when boys eat more sugar/carbs, they show less myopia development 3. This type of study has flaws in that it relies on questionnaire which can be highly subjective. In addition, many variables were not controlled, such as outdoor time, reading and screen time. Even if it’s to be trusted, the study like many epidemiological studies, evaluate a correlation, not causation. Besides, how do you interpret the data that sugar reduces myopia risks in boys? Would you recommend boys to eat more sugar and refined carbohydrates? I don’t think so.
In summary, little evidence exists to indicate sugar or refined carbs increase or decrease risks of myopia. Maybe this is just a factor that has not much to do with myopia. To advocate better oral hygiene and health, we certainly want children to control their intake of sugar and refined carbs, possibly for everyone really, not just kids. However, if you think that by eating less sugar you will not develop myopia, you are up the wrong tree.