When people think of inherited eye diseases, they usually imagine problems that show up in babies or childhood, with both eyes blind. But what if I told you the same rare eye condition can show up in kids as well as the elderly — and affecting two eyes differently?
Recently, I saw two patients who were diagnosed with a condition called Best vitelliform macular dystrophy, more commonly known as Best disease. Despite the name, it’s not exactly “the best” news to receive — though, thankfully, it tends to progress slowly and isn’t typically associated with total blindness.
Let’s start with the little girl. This is a sweet 6-year-old girl who failed school vision screening and referred to our clinic. She reports that she sees everything well, but parents note that she stays close to the TV to watch. After a detailed eye exam and specialized imaging, I diagnosed her with Best disease. She was otherwise completely healthy, with no complaints — though her vision is 20/60 in both eyes.
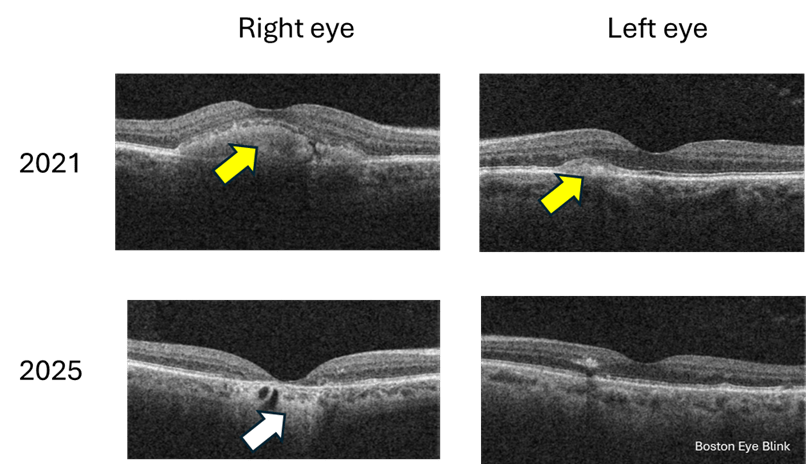
Interestingly, even though both eyes are not seeing well, they do show very different appearances in photos. Below is the color photo and cross-sectional view of her retina (Figure 1). Her right eye is at the ‘egg yolk’ stage, while the left eye has already progressed to the late, or advanced stage of macular atrophy. My heart goes out to the family. She is so young, and yet already at the late stage of this disease. Fortunately her vision is not too bad. And that is a common feature of this condition, that vision is typically only moderately impaired even in the late stage.
Figure 1. Photos of retina in a 6 year old girl with Best disease. The two columns represent right and left eye as labeled. A, color photo of the retina with subtle changes in macular appearance. B, autofluorescent black and white photo of the macula area. C, OCT cross-section photo of the macula in both eyes. Yellow arrow points to the ‘egg yolk’ in the macula of the right eye; white arrow points to a thin and atrophied macula in the left eye.
Then came the man in his sixties a week later. The two patients are not related. Just a coincidence that I would see two cases of a rare eye condition in the span of a week in a primary care setting. He started noticing blurry vision in the right eye when he was 50. He came to see us in 2021 but then lost to follow up. It gradually got worse, and now his right eye sees 20/40. His left eye sees 20/20 and no change over the years. Again, imaging confirmed the diagnosis. What is interesting is that you can see that over the 4 years, the right eye has progressed from the ‘egg yolk’ stage to ‘atrophy’ stage; while the left eye has little progression with still early or small ‘egg yolk’.
Figure 2. Cross-section macular photo of a 60 year old man in 2021 and 2025. Yellow arrow points to the ‘egg yolk’; white arrow points to atrophied retina.
So what exactly is Best disease?
This condition is so named not because it’s the best disease a person can have, it’s named after Dr Franz Best, a German ophthalmologist, who described the first pedigree in 1905.
Best disease is a rare genetic condition that affects the macula, the central part of the retina responsible for sharp, detailed vision. It’s caused by mutations in a gene called BEST1 [1], which affects a layer of cells beneath the retina called the retinal pigment epithelium (RPE). This layer helps keep the retina healthy and functioning properly. The prevalence is about 1 in 20,000 [2], so very rare.
The condition often runs in families and usually appears in childhood or adolescence, though some people — like my older patient — might not show symptoms until later in life. However, the adult onset Best disease may also be caused by mutations in genes other than BEST1 [1]. The onset of age ranges from 3-15 years of age [3]. It typically affects both eyes, though in some cases the two eyes show different rate of progression, which happens to be in both my patients.
Best disease is inherited in an autosomal dominant manner, meaning if there is one faulty gene, the disease will manifest. Therefore if one person has the disease, some of their family members are likely to have it too. But the degree and extensiveness of the disease can be quite variable among individuals [1], sometimes even with the condition, the person may not have any symptoms.
Interestingly, for both of my patients, they report no knowledge of any family history of low vision or blindness. I highly recommend the direct relatives to have a comprehensive eye exam with retinal imaging – the most important being the fundus imaging and OCT which can show cross section of the retina tissue. This technology can show the most striking feature, the yellowish lesion in the macula that looks a bit like an egg yolk — which is why doctors often call it a “vitelliform lesion.” You can see these lesions in the girl and the man in Figures 1 and 2 above. Over time, this lesion can change shape, break up, or leak fluid, leading to vision changes. In late stages, the macula becomes atrophied, meaning the tissue dies and thins out.
Can it be treated?
There’s no cure for Best disease, but the good news is that many people maintain useful vision throughout their lives. Regular monitoring is key to catching any complications early, especially if fluid builds up or if abnormal blood vessels form — in which case treatment might involve medications or laser therapy.
Recently, people are attempting gene therapy of this condition in dog models [4]. Hopefully gene therapy becomes available in the future in humans affected by this condition.
Why does this matter?
These two patients — so different in age and life stage — are a reminder that eye disease doesn’t always follow predictable rules. For example, Best disease usually affects both eyes, but these two patients both show remarkable asymmetry in stages of the disease. Best disease progresses slowly, and while it is true for the elder man, for the little girl, one eye is already at advanced stage. Given her young age, I imagine the progression has been fast.
And while it may not be “the best” diagnosis to receive, with proper care and awareness, patients can still live full, visually rich lives.
[2] Tripathy K, Salini B. Best Disease. [Updated 2023 Aug 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537290/
[4] Amato A, Wongchaisuwat N, Lamborn A, Schmidt R, Everett L, Yang P, Pennesi ME. Gene therapy in bestrophinopathies: Insights from preclinical studies in preparation for clinical trials. Saudi J Ophthalmol. 2023 Dec 1;37(4):287-295. doi: 10.4103/sjopt.sjopt_175_23. PMID: 38155675; PMCID: PMC10752275.
I recently saw a gentleman in his 70s due to double vision. He started seeing double vision 3 weeks ago at the airport. When he looked out of the window he saw two planes taking off though he knew there was only one. When he covered either eye, the double vision went away. But with both eyes open, he was seeing double images. But this was not happening all the time, only intermittently, and more when he’s tired.
He reported that similar double vision happened 15 years ago briefly, after he took some cold medicine, and it resolved on its own after he discontinued the medicine.
He did not recall any head or eye injuries. He did not have any other neurological symptoms. He felt well and did walking or cycling regularly. There was no history or family history of autoimmune conditions. He did have type 2 diabetes which was well managed. He had no history of heart disease or cancer. As for new medications, he remembered having covid-19 booster vaccine a month prior to the onset of double vision.
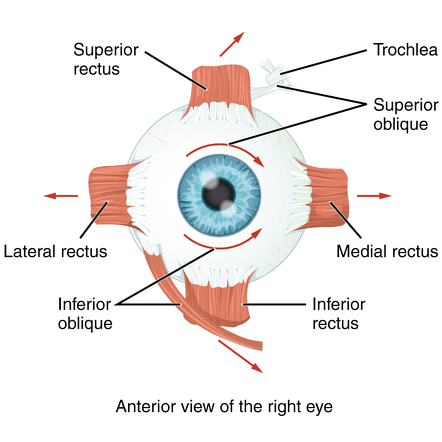
His history clearly indicated that his double vision was because the two eyes were not working together as they should. Many causes can lead to this. Each of our two eyes are controlled by 6 small muscles surrounding the eye (Figure 1). The two sets of corresponding muscles need to work in synchrony in order for the two eyes to look at the same object. If they don’t work in sync, double vision ensues. The first step is to find out which of the eye muscles are at fault. Because these muscles are in turn controlled by different nerves. Finding out which ones do not work will indicate which nerves are not working, and help to find out what is causing the nerve or muscle dysfunction.
Both of his eyes were able to move in all directions. I then did a careful measurement of his eye alignment, and found that he had a very small vertical misalignment between the two eyes. It was invisible by naked eyes, and only detected by doing an alternate cover test, in which each eye is alternately covered to show a deviation pattern. The result was that the left eye appeared to be slightly higher than the right eye. But it was such a small number and it appeared to be consistent in all directions where he looked. This is what we call a comitant deviation as it shows no difference depending on where a person looks toward. Having a comitant deviation usually indicates the problem has been chronic or benign. Further, the issue is not pinpointed to any specific eye muscle. Rather, multiple muscles may be involved.
The next step is to check if there are any other associated abnormalities. Pupil size differences or reactions to light often are altered in certain nerve disorders. He had normal pupils. Eyelid positions were also often abnormal with some of the nerve problems. His eyelids were symmetrical and both slightly loose and droopy normal at his age.
His vision in each eye was stable, and he just saw another eye provider for a dilated eye exam not long ago with no remarkable pathologies.
So I thought this was a decompensated phoria issue. This means that the person has a slight misalignment between the two eyes and usually well compensated; in certain situations, for example, when tired, stressed, or aged, the compensation reduces and they start seeing double images.
While he was in my office, he was actually not seeing double, indicating a good compensation. Still, since he did frequently see double for several weeks, I offered to try some prism to alleviate the problem. Prism changes the direction of light, and can therefore allow two eyes see the same image if light direction is altered just matching the misalignment. He felt seeing things more clear and comfortable with 1 unit of prism. Interestingly, he felt comfortable and clear with up to 5 units of prism before he complained of seeing double at 6 units. This type of a relatively large range of fusion often indicates a congenital misalignment. The most common being congenital cranial nerve 4 palsy. However, this did not appear to be what he had, as he had no head tilt now or in his driver’s license photo, and the comitancy of the misalignment that we discussed earlier also did not fit.
This was not a typical case. It was not likely from a brain etiology, but some of the mimickers that can cause double vision should be ruled out. So I ordered blood tests for myasthenia gravis and thyroid eye disease. I prescribed prism glasses and asked him to follow up in a few weeks.
To my surprise, a few days later, his blood test was positive for myasthenia gravis (MG), an autoimmune condition that weakens the communication between nerves and the muscles they control. I immediately referred him to a neurologist, the speciality that diagnoses and treats this condition.
The neurologist concluded that he had the ocular MG, which affects only eye muscles. However, with time many patients with ocular MG may convert to generalized MG, with muscle weakness affecting other organs of the body. The most serious would be the muscles for swallowing and breathing, as they may develop difficulty breathing, which can be life-threatening. Further, a subset of MG patients also have a tumor in their chest, called a thymoma, and 30% of these tumors are malignant. So my patient is going to have a chest CT very soon.
I saw him again for follow up and he reported seeing well with the new glasses and did not have double vision any more. With ocular MG, the double vision could change pattern over time so we would monitor this regularly. Given that he had no other symptoms, no additional treatment was necessary at this time and he was also being monitored by the neurologist regularly.
My patient does not require additional treatment besides prism at the moment, but if his symptoms change, additional treatment may be necessary. For example, medications such as pyridostigmine, oral steroids, immunosuppressive agents, intravenous immunoglobulins (IVIG), and biologics. When difficulty breathing develops, patients should go to emergency room to have prompt IVIG treatment as it can be life-threatening.
MG can present in the eyes first. In fact, almost 50% of MG present as ocular MG [1]. But up to 60% will eventually convert into generalized MG [1]. One classical feature of ocular MG is the incomitancy of double vision, which we discussed above. This means that double vision or the misalignment of the two eyes is different depending on which direction the person looks at. As you recall, my patient had comitant deviation, which was why it surprised me that he tested positive for MG in the blood test. However, it’s a relief to find in literature that 25% of ocular MG were reported having comitance or change of comitance to incomitance or vice versa [1]. Further, another classical presentation of ocular MG is ptosis, or droopy eyelid, which my patient also did not have. MG diagnosis is often delayed in cases where there is only double vision and not ptosis.
Another interesting observation is that there were multiple reports of new onset MG shortly after covid-19 infection or vaccination [1]. However, a causal relationship was not well established. I did not think twice about his covid booster, but seeing that this is observed in the scientific community, I will probably ask about covid infection of vaccination in future suspected MG patients.
Lesson learned is that even an atypical case of double vision could be MG. Having no ptosis does not mean it cannot be MG. Being comitant in double vision does not mean it’s not MG. Don’t ever forget to rule this condition out.
For more information, please refer to this excellent review article [1]. Direct references and much more information about ocular MG can be found in there.
Review article cited:
[1] Behbehani R. Ocular Myasthenia Gravis: A Current Overview. Eye Brain. 2023 Feb 5;15:1-13. doi: 10.2147/EB.S389629. PMID: 36778719; PMCID: PMC9911903.
I look at eyes all day, and have to admit that I care less about anything else. But this case was a big help from another specialty which not only nailed the diagnosis but also saved a lot of $$$ and time on the expensive and lengthy tests that we so often have in the health care.
Case: visiting the eye doctor
A man in his mid 50s, Edward, we will call him, came into the office complaining about new floaters in the left eye for 1 week. This is a very common complaint, which I hear about almost daily.
If you read my previous posts, you would know that the most common cause of floaters are vitreous degeneration or detachment (link and also here) and the biggest worry would be that there was a retinal tear or detachment in the process (Refer to Figure 1 below for these structures: vitreous and retina).
He saw no flashes, and there was no injury to the eyes or the head. He had no pain and no visual changes.
The exam showed normal vision, normal eye pressure, and interestingly no vitreous detachment. However, there were some cells in the vitreous in the left eye (again refer to Figure 1 to see where the vitreous is in the eye). The retina appeared normal without any tear or detachment. A closer looked showed that there were even cells in anterior chamber, the front chamber of the eye (in contrast, the vitreous is the back chamber of the eye).
Figure 1. The vitreous is a large space filled with a jelly inside the eye. In Edward’s case, this jelly now contains many inflammatory cells causing him to see floaters. Image from National Eye Institute [1].
So this was a form of uveitis, which is less common, but also can cause floaters, which I talked about in a previous case also (link).
Uveitis is the inflammation of the colored layer of the eye, called uvea (Figure 1). Injuries can cause this inflammation, but so can infections, autoimmune diseases, cancer and sometimes no reason that we can find.
The question is, what is causing the uveitis?
More about this patient
I asked him if there was anything else going on besides the eyes?
He said, ‘I have had a skin rash on my back before the floaters showed up. My dermatologist gave me a fungal cream but it’s not working and I am going back to see him next week.’
Otherwise he was in his usual health with no complaints.
Looking at his other office visits, I could see that he fought two cancers, once 10 years ago and once 5 years ago. Fortunately both were found in stage 1 and adequately treated.
He was HIV positive, but had normal CD4 values and was taking his anti-virals consistently. He was also being tested regularly on chlamydia and syphilis and negative in these in the last labs 4 months ago.
Based on this history, cancer is a concern. But HIV related etiologies are also possible. These both can cause uveitis. Further, inflammatory causes (non-cancer, non-infectious) are also possible.
Cause of uveitis revealed by skin test
I promptly referred him to our uveitis specialist, who will run a battery of tests and imaging to figure out what is the cause.
However, it was his dermatologist that nailed the diagnosis and sent him for the definitive treatment.
Since the rash did not improve with medical treatment, his dermatologist performed a skin biopsy, which showed a very small bug (called spirochetes), the causative agent for the rash, and also the uveitis in the eye. These spirochetes are the microorganisms that cause syphilis, a sexually-transmitted disease that is sometimes found to be more prevalent in those with positive HIV.
In this case, a simple skin biopsy saved him the trouble of a battery of tests and imaging procedures, which was the silver lining of his unfortunate symptoms. The treatment, IV penicillin, is usually quite effective.
Additional thoughts
In the end, this outcome might be the best it can be. Cancer in the eye, such as lymphoma, would be much more difficult to get rid of, not to mention possibility of death.
As an eye doctor, the most important thing is not to mis-diagnose this special form of uveitis as the good old vitreous detachment, even though vitreous degeneration or detachment is the horse, and uveitis is the zebra.
And syphilis, a great mimicker of all forms of uveitis, should always be tested, especially if the patient is at risk.
So if you have new floaters, please reach out to an eye doctor, because your retina may be at risk and it could be something else.
Learn more about uveitis from this reference below.
This is a case where two rare eye conditions happen to the same patient, as if they win the lottery (of the unfortunate) twice.
I saw Mary (not her real name) in her early 50s last year. She came to me because she had seen new floaters in the left eye for 1 week. I have written about floaters previously, you can find them here, here, and here for more information.
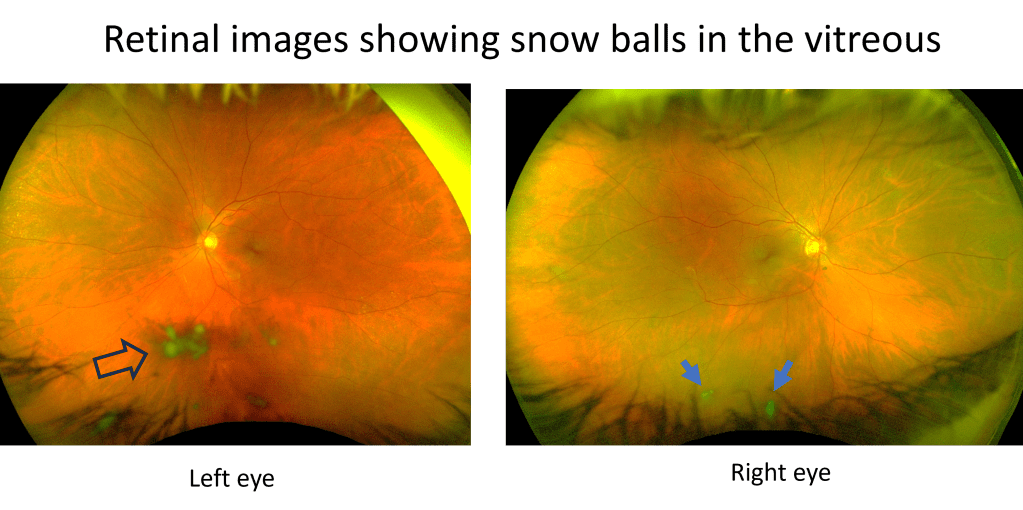
There are floaters that affect almost everyone: the regular floaters and the acute PVD (posterior vitreous detachment) floaters, and there are also weird floaters that affect only a few who win a lottery in the weird eye condition category. Mary won that lottery unfortunately. There were snow balls in her left eye, inside the jelly we call vitreous. You can see these snowballs when looking at her retina (Figure 1).
Figure 1. Initially only the left eye had intermediate uveitis, with snow balls (immune cells aggregates) in the vitreous as shown by the arrow head on the left; months later the right eye also developed intermediate uveitis with snow balls as shown by two arrows on the right.
This is called vitritis, an inflammation of the vitreous (which is the jelly inside the eyeball). When vitritis happens alone without inflammation in other parts of the eye, it is called intermediate uveitis. The most common symptom of intermediate uveitis is floaters. The snow balls are actually the immune cells accumulating inside the vitreous. It is critical we find out why inflammation happens there, because some of them can have serious health consequences to a patient’s vision and even life.
Common causes can be infections such as tuberculosis, leprosy, Lyme’s disease, syphilis, toxocariasis; autoimmune diseases such as sarcoidosis, multiple sclerosis, inflammatory bowel disease, Sjogren’s disease, tubulointerstitial nephritis and uveitis (TINU) syndrome; and cancer such as lymphoma.
I referred Mary to a uveitis specialist, who did an extensive workup and did not find a cause for her intermediate uveitis. This happens more often than not in medicine. But at least the infectious causes had been ruled out, so immune suppression treatment can be started; if the cause is an infection, then immune suppression will make things worse. She was started on oral steroids to treat the presumed autoimmune cause (though unclear what it is. She saw a rheumatologist but no diagnosis was found). She got better, but vitritis returned after the steroid taper. At that time they also found increased transaminase indicating a liver problem so no more oral steroids were given. She saw a GI specialist, who did not find a cause of increased transaminase level, and a few months later the level got better on its own.
Given the potential liver issue, no oral steroids, but eye drop steroids were given to her to treat the vitritis. She got better for sometime, but then her eye pressure spiked as a side effect of the steroid eye drops, which had to be discontinued. Meanwhile vitritis started in her right eye as well (Figure 1).
Next step of treatment would be a systemic agent that does not cause liver damage. The uveitis specialist was able to get insurance to pay for Humira (Adalimumab), and with this medication, her vitritis and floaters finally got better in both eyes up until now. This medication blocks the activity of TNF, a molecule used by our body’s immune system to create inflammation. Less TNF means less inflammation in the eyes, and it has been working for her.
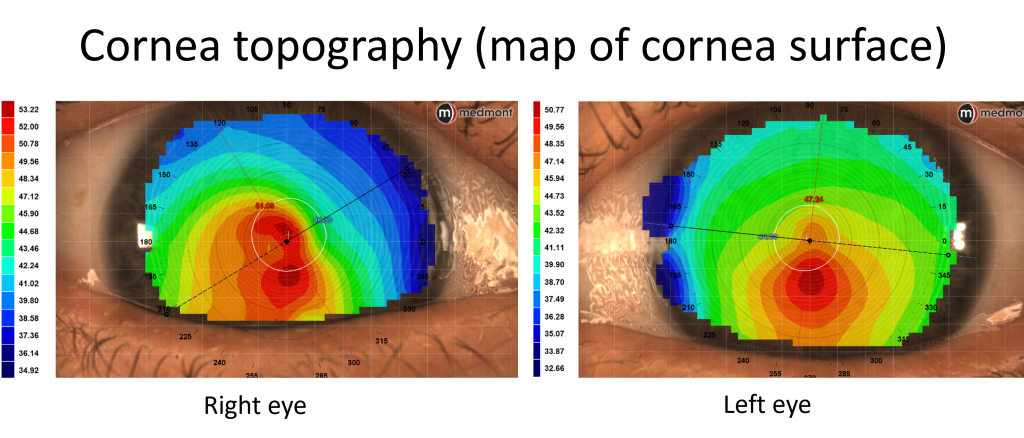
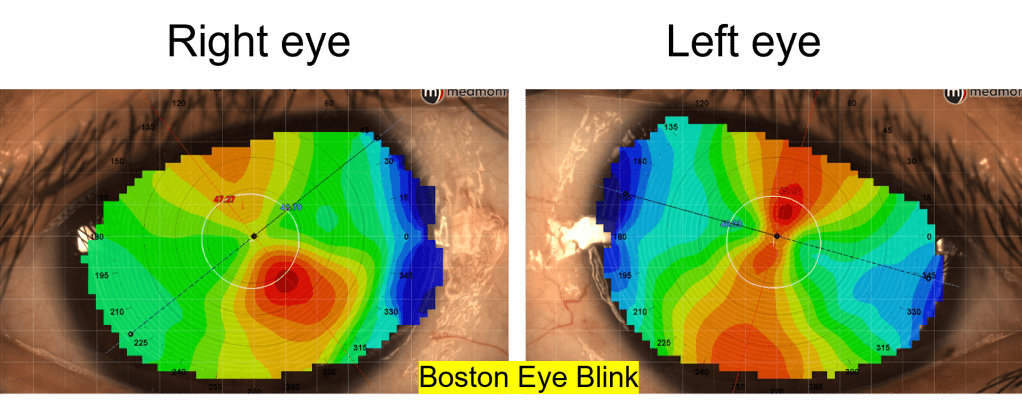
She came back to me again for new glasses now. A year ago when she first came to see me, she was wearing her new glasses of just 3 months. She had myopia and astigmatism in both eyes, more in the right eye. In that visit 1 year ago I actually found more astigmatism in the right eye and gave her an updated script. It was a little unusual to have a change in just 3 months, but she had other things to worry about for her eyes (the vitritis), so this was not pursued. Now her vision was blurry, and the right eye had a further increase in astigmatism. This is not normal. So I ordered a corneal topography, and sure enough, she actually has keratoconus in both eyes (Figure 2).
Figure 2. Surface map showing steepening of inferior cornea (evidenced by red color) in both eyes, characteristic of keratoconus.
Keratoconus is not a common eye condition, and you can read about it in my previous articles here and here. It often shows up among young people, as the disease tends to progress at a young age. For her to progress and get a diagnosis at 53, that was unusual. Talking about coincidences, I happened to have another 52 year old female patient on that same day whom I diagnosed keratoconus 6 months ago. She also started having vision problems only in the recent couple of years. Life sometimes cannot be explained by just random events, or we humans are just too good at picking up anomalies.
Anyway, the prevalence of intermediate uveitis is very low, about 6 out of 100,000 people. The prevalence of keratoconus is higher, about 5%, but still not a common condition. For her to have both, it is a chance of 3 out of 1 million. Winning two lotteries!
I would not want her luck. Getting either one of these conditions is a frustrating journey in gaining vision back. She is frequently in doctor’s offices, taking eye drops and medications probably life-long if she’s lucky enough to have the eye inflammation under control, may need eye surgeries and special contact lenses if vision continues to worsen with keratoconus.
After the new measurement of her eye powers, I gave her a new prescription. She was happy and said, ‘I haven’t had new glasses for over a year, now I’m ready to get new ones and see better.’ In fact, she sounded more positive than many of my healthy patients whose only problem was needing glasses. Happiness is a state of mind, regardless of the conditions that you may have physically.
I received a message from a patient who sounded desperate. She said that her eyeball is changing color, that she has necrotizing scleritis, and her uveitis doctor is not picking up the phone.
The last time I saw her was a year ago, she was only 22, a young and vibrant age. However her lazy eye was bothering her a lot. She had it since she was a little baby, the right eye went out with poor vision. She had patching therapy to treat lazy eye, but her vision was still 20/100 in that eye at its best.
Lazy eye is a condition that develops before 8 years of age. From birth to roughly 8 years, kids’ eyes need to receive sufficient visual stimuli to develop their visual pathway leading to normal vision. A lazy eye could be turning out or turning in, or turning up or down, which prevents this eye from getting the proper visual stimuli, leading to abnormal development of the visual part of the brain corresponding to this eye. As an adult, it becomes very difficult to treat lazy eye, as the visual brain becomes less elastic.
Not only does a lazy eye that has an eye turn affect vision in one eye permanently, it also poses a psychological and social challenge for patients. A very noticeable eye turn can cause reduced self esteem and is a problem beyond just the cosmesis. Many adults with an eye turn seek surgery to make their eyes appear straight, even if that does not change vision. When I asked if she was interested in such an option, she very happily said yes.
So I referred her to a specialist that does such surgeries for adults.
Most of these surgeries are successful, with a happy patient who feels more confident in their daily lives. Complications are uncommon.
The surgery went well for her. However, very unfortunately, a rare complication happened. Necrotizing scleritis is a rare eye condition which can be caused by autoimmune conditions. She has a preexisting autoimmune condition, psoriatic arthritis. With this condition, patients have joint pain and red scaly rashes on their skin. Her symptoms were in good control prior to the surgery. However, unfortunately the surgery and sutures triggered inflammation of the white lining of the eyeball, the sclera. Remember she has only one good eye with the other seeing poorly from being a lazy eye. Though eyes are straight, she still relies on only the good eye to see and function. The unfortunate part is that the good eye developed the necrotizing scleritis, as eye turn surgery was typically done on both eyes. Scleritis is a rare condition, necrotizing scleritis is even more rare. It is the most severe form of scleritis, with the tissue undergoing necrosis, or death. Patients have excruciating eye pain and reduced vision. The prognosis is poor, with high likelihood of vision loss.
No one could foresee such a complication to happen, but it happened. She was seeing uveitis specialists from the best eye hospital in the area, as well as rheumatologists. The silver lining of this unfortunate event is that after some time, her eye was stabilized and under control with a medication called methotrexate as well as multiple eye drops. She was doing well for some time and her vision was preserved.
Until she got pregnant. She should not get pregnant while taking the medication that she’s taking for her active autoimmune condition. It was not planned. But she’s happy with her fiance and she’s scared but loves her baby. Methotrexate is a pregnancy category X drug, which means it is not recommended to take during pregnancy. It may cause miscarriage and birth defects of the baby.
What now? She had to stop the medication. Her eye condition took a turn. It’s getting worse again, and she is being referred from one uveitis specialist to the next. She was not able to get an appointment and she told me that her eyeball is changing color. The color change in scleritis means the sclera tissue is getting thin, to the point the underlying choroid is showing through.
I am not a uveitis specialist, her case is beyond my specialty. I reached out to her specialists- I do not want to get into the details of the process- and I believe that she will be seen and treated soon.
It is not easy to be a woman. First off, women are more likely to have autoimmune conditions and more likely have severe symptoms. Well she is one of these women. Autoimmune diseases can affect young people, and she is young. Second, most medications for autoimmune conditions are not pregnancy friendly. For women at child-bearing age, if they are battling active autoimmune diseases, they hardly have a choice to have kids. If they do get pregnant, they may have to hold off the treatment and risk their conditions getting worse. There is no winning for them.
For my patient, she has bad luck to incur a rare complication after a usually very safe surgery, a surgery that she rightfully deserves. The pregnancy should have been prevented. But accidents can happen. On the one hand, she is risking losing vision in the only good eye without the medication, and on the other, she would be risking the baby if she were to resume the medication. Difficult choice and I feel very sorry that she has to choose.
The mysterious case of poor vision with contact lenses
A 38 year old guy came to see me to check his contact lens prescription. He got the final contact lens prescription from another optometrist in our practice in March, so about 8 months ago, and he could no longer see well with them. This is a red flag. In adults, prescriptions are typically stable for years. 20-40 is a stable and healthy period for the eyes, with relatively few diseases and certainly few fluctuations in refractive power of the eye. But our patient obviously has a problem despite his young, primal age. So let’s look at what’s going on.
He’s wearing biofinity Toric XR lenses. For those of you who are not familiar with it, this is a monthly disposable contact lens that corrects for high amount of astigmatism that most other regular contact lenses do not correct. Toric lens is a lens that corrects for astigmatism. Astigmatism is when the eyeball is not shaped perfectly like a soccer ball, but rather a bit like the American football, so different in terms of curvature on the two different planes. And that’s why people can get blurry vision with astigmatism and there are certain contact lenses, the toric contact lenses that can correct this. Right now his contact lens prescription is about -8 – 3.5, that means he has about 8 diopters of myopia as well as 3.5 diopters of astigmatism. As you can see that’s a lot. When I look at this previous record from March, he was wearing these contact lenses and his vision was about 20/30 with the correction. So that was not 20/20 either. And 20/20 is usually the standard healthy vision that we’re aiming for. Anyone without a notable disease of the eye should have the standard 20/20 vision, especially adults. Today his vision with the contact lenses is only 20/100 and he has over these contact lenses a very large prescription, another five diopters of astigmatism. That is really striking difference, and that should not happen with healthy eyes.
When I asked him, he reported that even when he first got the contact lenses, he was not really seeing all that well. And now it’s getting progressively much, much worse, to the point he could no longer work and it was difficult to drive. I asked him, “Are you sure you put the contact lenses in the right eye?” Sometimes patients would mistakenly switch the contact lenses for the two eyes and that can make things a little funny as obviously the two eyes will be using the wrong prescriptions for both of them. He said that he made sure of it. In the past, he did accidentally switch the two lenses and it was very blurry. He was able to recognize that and switch them back, and now this he was very sure he was using the right lens in the right eye.
I asked him to take off his contact lenses and started doing refraction again. It turned out he could not really see that well even with the new prescription. And the new prescription was markedly different than his current prescription back from March as well. So his glass prescription has also changed a lot. This is very strange. At this moment I was suspecting something funny on the surface of the eye because he does not have diabetes, which is another common cause of large refractive changes over a short period of time. A really quick way to test this is to check the red reflex on retinoscopy. I took up the retinoscopy scope, and this is a light that you can shine into a patient’s eyes and the red reflex would show up funny if there is anything irregular on the surface of the eye. However, nothing wrong showed up there.
I then took a look at his eyes under a microscope, a slit lamp. This is a lighted microscope that you can magnify and see fine details of the eye. I was looking at the surface of his eye and it looked really healthy. There was no notable dry eye. He’s got healthy tears as well. His cornea is completely clear and there’s no staining on them. There’s no opacity on the cornea.
I didn’t dilate his pupils and check the back of the eyes immediately. I could put some dilating eye drops in and check to see if there’s any disease in the middle or in the back of the eye. But I didn’t do that. With the dilation you have to put the drops in and that takes about 20 minutes for the pupils to get bigger. And patient’s eyes remain dilated for the next four to six hours. It can cause a lot of inconvenience. Obviously when it’s necessary, we have to do this. But he’s got to work afterwards and doesn’t want to get dilated.
So the next high yield exam is a corneal topography. This is a machine that draws a map, a very fine, high resolution, accurate map of the surface of the cornea that you may not necessarily see with just the magnifier or with a retinoscope. This test is quick. You just need to turn the machine on, patient looks into a bowl of concentric rings, and it takes a few seconds to take a picture for each eye. A minute later, it becomes apparent that there is something wrong going on in the corneal surface that I am not able to see with the other techniques. It is not very obvious. It is kind of subtle, but he’s got a condition called keratoconus. Figure 1 shows his corneal topography findings.
Figure 1. Corneal topography map of definite keratoconus in the right eye and possible keratoconus in the left eye.
What is keratoconus?
Keratoconus is a condition that affects the cornea of the eye, and cornea is the very surface of our eye, the clear thin membrane covering up the surface of the eye, and through that clear cornea you can see the iris, which is the colored part of the eye, as well as pupil, which is the small opening in the center of the iris. The front surface of the cornea is very important. If there’s anything irregular going on, your vision can be blurry. In keratoconus, the cornea undergoes degenerative changes through the years. It can happen very quickly over a short period of time, but it can also stay dormant for months and years. Keratoconus happens in about 1 in 700 people in the general population. So while it is not extremely common, it is also not a rare disease.
This is unfortunately a disease that affects the young people. Children as young as eight years of age can start developing keratoconus, but typically it happens in late teenage years and it can continue to get worse through the years. It happens to both eyes, but it can be asymmetrical, meaning one eye may be affected more. I’ve seen many people who have one eye completely normal 20/20 vision do not need glasses. The other eye with relatively advanced keratoconus.
But even in this apparently normal eye, if you do the corneal topographer map like what I did for the patient, you could see some problem for the normal eye. The apparent normal eye may also have sign of very mild keratoconus that’s fortunately off center- it’s often inferior, that means in the lower part of the cornea so it’s not in the visual axis. That’s why patients can see well, it’s not affecting their vision. But nonetheless, the disease is there and it may be dormant in the lifespan of a person, but it can also start progressing anytime.
Who are affected by keratoconus?
The cause of disease is still not clear, but people have seen that this runs in the family. Of course, it can happen to someone who has absolutely no family history of keratoconus, and it just starts with them. Or you can have parents with keratoconus, but the children can be completely normal. The genetics of this is not completely figured out, although some company is selling genetic tests for this condition.
It is believed that changes in the enzymes of the cornea are undergoing changes, bad changes that break down the collagen of the cornea. There are several layers of the cornea and some of these layers are fragmented and also becoming much thinner. There is sometimes a break or folds in these layers, and that also can lead to scarring and making the cornea very cloudy.
People have observed a few things that are associated with keratoconus. One of them is rubbing of the eyes, and many doctors believe that the rubbing mechanical action on the cornea itself can make it change in shape, thinner and make lose its normal property. And that certainly has its merits. Except, many keratoconus patients actually don’t rub their eyes. Some of them do, and they often have other conditions like allergic conjunctivitis. Their eyes are always itchy or dry and they feel uncomfortable and hence they always rub their eyes and that does make keratoconus worse. But many people actually rub their eyes a lot, but never develop keratoconus. This patient denies rubbing his eyes. He denies having itchy eyes or irritable eyes. And the surface of his eye as well as his conjunctiva do look pretty healthy. There’s no sign of inflammation there, so I have no reason to believe that he is lying.
Another association people have observed is that those with Down syndrome sometimes have keratoconus. Although, in my experience as a primary care optometrist, many Down syndrome patients have perfectly healthy corneas and majority of my keratoconus patients don’t have Down syndrome.
And another condition that’s associated with keratoconus is Ehlers-Danlos syndrome, a connecting tissue disorder. It kind of makes sense that their cornea would be weaker because cornea is made of collagen, which is the component of connective tissues.
Some risk factors have been proposed for keratoconus, including number #1 eye rubbing. And #2 is sleep apnea and this is an interesting one. Now with sleep apnea there is another highly associated condition, floppy eyelid syndrome. These patients’ eyelids are pretty loose. And when they sleep, they sometimes can inadvertently flip their eyelids and their cornea can be exposed to the pillowcase, resulting in corneal injury and eye pain in the morning. So connective tissue disorders may be the underlying cause of floppy eyelid syndrome as well as sleep apnea, and that could also be the underlying cause of keratoconus.
Retinitis pigmentosa can also be a risk factor for keratoconus. This is a condition that I will talk in details another time.
Why is keratoconus sometimes missed by eye doctors?
It is not easy to diagnose keratoconus, especially in the early stage. Like I mentioned, I try using retinoscopy and that’s one way to diagnose keratoconus. Typically you would see a scissor reflex when you do the retinoscopy procedure. There are two lines crossing with each other. However, that may happen in intermediate or above level of keratoconus. In early stage it may not show up that well.
Other methods include a slit lamp exam. Sometimes you can see folds in the deeper layer of the cornea. Sometimes you can see scarring and obviously that’s a much later stage and patients typically already see poorly before that. So that’s not really useful to diagnose early keratoconus. Sometimes you can see thickened nerves. Corneal nerves are typically not obviously visible even with the magnifier, but in keratoconus, for some reason the coroner nerves can be thickened. However, this is not a specific test for keratoconus because some normal people can have thick corneal nerves. Sometimes people can see a ring that is an iron deposit present within the epithelium of the cornea around the base of the cone. But it is also not always seen, especially those with early keratoconus.
People often classically cite Munson sign as a sign of keratoconus. That is a protrusion of the lower eyelid in downgaze, because in advanced keratoconus the surface of the cornea becomes almost like a cone, and so you can see that when people look down with that cone touching their eyelid, that is advanced keratoconus. You certainly do not see that in the early form.
So many of these are helpful, but none is the definitive sign of keratoconus, or they’re often not present or not obvious in early keratoconus.
To diagnose keratoconus, you really need to have high clinical suspicion and order that corneal topography test. This test is highly sensitive and it does show keratoconus much earlier than many of the other clinical exams. Classically in a corneal topography map view you will see steepening, which is usually indicated with red color whereas normal curvature is indicated with the green color. If you see the red color in the lower part of the cornea, that’s highly suggestive keratoconus. In early keratoconus, though, that redness may not be very obvious, and you have to rely on the asymmetry of the steepening of the cornea from the upper part of the cornea as well as the lower part.
In my patient, you will see that he has a lot of corneal astigmatism. So there’s redness both from the upper as well as lower part, but the lower part of the map is much more steepening than the upper part (Figure 1). This asymmetry is also a characteristic to differentiate from a regular corneal astigmatism, that would be equal amount of steepening from both the upper and lower that would be symmetrical (Figure 2) and that would not affect vision as much. And patients typically would see well with glasses correction and obviously with the contact lenses they would see well. A corneal map of more advanced keratoconus is shown in Figure 3.
Figure 2. Corneal topography map of regular astigmatism. This patient has high degree of astigmatism, but it’s regular, hence good vision with glasses. Note the symmetry between the red areas for the upper and lower halves in both eyes.
Figure 3. Corneal topography map of a patient with intermediate to advanced keratoconus. Note the red area is only evident in the lower half of the cornea, that is, the marked asymmetry between upper and lower halves in both eyes.
The corneal topographer in our practice can only capture map of the front surface of the cornea. There are some topographers that are able to map the back surface of the cornea as well. In keratoconus, it is observed that the earliest changes actually happen to the back surface of the cornea, before any visual symptom even shows up. If you go for a LASIK surgery evaluation, they will use this type of corneal topographer, because LASIK surgeons really want to catch the most hidden form of keratoconus as it’s a contraindication of LASIK surgery, more about this later.
Another reason eye doctors won’t think twice when giving out a new stronger prescription to a young person is the myopia epidemic. Myopia progression can produce the similar phenotype with kids updating their glasses every 6 months. Both conditions affect young people and myopia is so prevalent these days. Please check out my articles on myopia and myopia control. Sadly, myopia progression and keratoconus can certainly happen to the same person.
Patients with keratoconus typically have a history of good vision with glasses, just like those with myopia. Gradually their glass prescription changes over the course of years, until eventually, even with very high prescription of glasses they could not see well. They would turn to soft contact lenses that would work well for a period of time, but then vision may get worse again, until eventually the diagnosis of keratoconus is made.
What are the treatments of keratoconus?
And that’s the time when we should address this issue. And not just treat the symptoms, but actually treat the disease itself. Although this can be a degenerative condition that progresses overtime, there’s no inflammation associated with it. So anti-inflammatory treatment or medication will not be able to help in this condition.
The treatment of keratoconus comes in several different ways. First, we want to address the underlying cause. Without the treatment, keratoconus can be progressive, so early diagnosis is key. Once you diagnose the condition, you can start a treatment called corneal cross- linking to strengthen the cornea and stop the disease from progressing further. This procedure was approved by the FDA in 2016, so not that long ago, but it is the only way that can actually stop the disease from progressing. Note it does not reverse the disease, so it does not make the cornea better, or make the vision better. Patients will still need contact lenses and glasses to see better after the procedure. The cornea cross linking procedure really strengthens the cornea and renders the corneal stable from undergoing further degenerative changes over time. In this procedure, the corneal epithelium is taken out first and you would soak the cornea with drops of riboflavin. Then the cornea is exposed to UV light for 30 minutes. During this process the collagen inside the cornea will cross-linked with each other, therefore rendering the structure more stabilized. After crosslinking, when the eyes are stable, you can use contact lenses and glasses to see better. There will not likely be further change of prescription after this procedure.
Vision in keratoconus often cannot be corrected with glasses because the surface of the cornea itself is irregular. Regular soft contact lenses also cannot correct vision to a satisfactory level. Again, because any soft contact lenses put on the eye will drape over the irregularity. So the only way that allow more than mild keratoconus patients to see a little better would be a hard contact lens, whether it’s a small hard corneal lens, called a gas permeable (GP) lens, or a bigger hard lens called the scleral lens. These hard lenses will be able to mask the irregularity of the cornea and provide clearer vision. I have prescribed a lot of both types of lenses to keratoconus patients which make them see better again. Just yesterday a patient told me ‘I have never seen this well for a long time”, after he tried on a special GP lens.
The corneal gas permeable lenses are small, clear plastic contact lenses on the surface of the cornea, so it covers the black part of the eye only, and it can move freely whenever you blink. There’s a tear layer behind the lens as well as in front of the lens, therefore masking the irregularity of the cornea. It’s relatively easy to put in and take out, and easier to care for, but in the beginning of using the lens, many patients reported their eyes hurting with foreign body sensation, especially with blinking. And that’s understandable, because after all, you’re having a hard piece of plastic inside the eye that certainly is not comfortable. Fortunately, most patients get used to them after a few weeks of using the contact lens.
Scleral lenses are much bigger contact lenses. They are sort of like a small bow that hovers over the entire eye, so it actually touches on the white part of the eye. Therefore it does not hurt as much. In fact, it is quite soothing. You almost don’t feel that you have a lens inside the eye. You would fill the bowl of the scleral lens with preservative free saline, so from that aspect it is soothing to the surface of the eye. This lens is comfortable. It also corrects the irregularity on the surface of the cornea. However, the disadvantage is that it is much more expensive and it is a little more difficult to care for. And it is also more difficult to learn how to use it as you have to use a plunger to apply the contact lens inside the eye as well as the plunger to take it out. So the learning curve is a bit steep for patients.
As with any contact lenses, the corneal gas permeable contact lenses as well as the scleral lenses need to be carefully cared for and patients should never sleep in these contact lenses, they should always take them out before going to bed and soak them into the correct disinfectant solution and to be used again the next morning. Before touching the contact lenses, patients should always wash their hands with soap and water and make sure not to touch the lens with dirty hands. Patients should not go swimming, taking a shower or sleep in contact lenses.
Medical treatment sometimes is needed. A complication can sometimes develop in keratoconus called acute hydrops, this is a condition where a break develops in the inner layer of the cornea, allowing the fluid inside the eye to enter into the corneal stroma, causing severe edema and thickening, light sensitivity, decreased vision, tearing and pain. And this needs to be managed acutely because Hydrops can lead to corneal scarring. Providers will need to try to manage the pain and swelling. We can give patient a dilating eye drop that reduces the pain. We can give patient sodium chloride 5% ointment, which can reduce edema and improve vision a bit. It may take several weeks for Hydrops to completely clear. The patients may need to use this ointment for weeks or months before it finally resolves.
Unfortunately, sometimes advanced cases can occur. Corneal scarring can occur that no contact lenses will be able to restore vision, and to that end a corneal surgery needs to be done. A new cornea transplant can be placed in to replace the keratoconus cornea that has scarring.
Why is keratoconus an emotional eye disease?
I think keratoconus is a frustrating disease. It affects young people who have been seeing well in first two decades of life. And slowly their vision starts to get worse and this change, especially when early, is often missed. So they end up going to the eye doctor’s office a lot with multiple pairs of glasses with constantly changing contact lens prescription. And with frustration that their vision continues to get worse, if lucky and it is diagnosed early and cross linking is done, the cornea can be stable and hopefully patients can see much better to a normal level with the proper contact lenses or glasses, but many of the keratoconus patients need to use specialty contact lenses for all their life. To them, contact lenses are not an option. They have to use them simply because glasses will not make their vision good enough. They have to take care of the contact lenses all their life. That is a serious commitment. You have to follow all the rules. They’re not really good candidates for LASIK surgery. And in fact, sometimes latent keratoconus can become pronounced after a LASIK surgery procedure. I have seen multiple patients who develop keratoconus after LASIK surgeries. Although nowadays people are starting to do LASIK surgery together with cross linking and this may hold to be a promising procedure for keratoconus patients in the future that they may have surgery to correct their vision and do not have to worry about complications to their cornea.
Conclusion
To recap, early detection and diagnosis of keratoconus is really key in managing this disease. Once diagnosed, crosslinking procedure should be recommended. Even though most keratoconus progression happens before 40 years of age, I have seen patients that are progressing well after 45 years of age, so a cross linking procedure should be highly recommended to any patient if it’s still progressing, no matter their age. Hopefully keratoconus patients in this day and age can be diagnosed early enough with early intervention to prevent the need of significant corneal scarring and corneal surgeries, and hopefully glasses and contact lenses are all they need. Any young person with unexplained vision reduction should have the benefit of taking a corneal topography image to rule out keratoconus.
Today I will tell the story of a patient who lost half of his vision.
Disclaimer: patient’s name is an alias, but the case is real.
I saw John once a year for a few years, monitoring his glaucoma suspicion. Glaucoma suspicion simply means that one’s suspected to have, but does not really have glaucoma yet. He had good vision in general, but usually had many complaints about his vision, mostly that he had to use glasses which he never needed to wear before.
Once he splashed some chemicals in his right eye while doing house work, and saw my colleagues multiple times while I was on vacation. According to the medical record, the chemical burn had resolved. He came to see me shortly after that.
‘Doc, I cannot see with my right eye’. My thought was, maybe he was having scars on the cornea. But his cornea looked clear with only a faint scar in the periphery that could not cause vision loss. What’s also interesting was that both his eyes had similar vision. But he insisted that since the chemical splash, he could not see well in the right eye. Could the chemical have reached the back of the eye and caused retinal or optic nerve damage? With a dilated exam, as well as photos of the optic nerve, everything still looked as good as before. There was no apparent retinal or nerve damage.
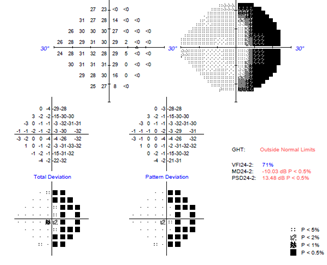
So I ordered a visual field test. This test examines the periphery vision rather than central vision. I have a couple of his results from previous glaucoma testing, and one looked like Figure 1 A. The dark spots mean vision is less sensitive in that region. So in this graph (Figure 1A), there are only a few minor defects in both eyes.
Figure 1. Gray scale graphs representing visual field results. Each eye was tested separately and darker the spot means worse vision in that particular region. Copyright: Boston Eye Blink
When I saw his visual field results on that day (Figure 1B), I knew the worst had happened. I immediately called him and said, ‘John, you have to go to the emergency room right now.’
As you can see now he had lost a half of vision on the right side, both for right and left eyes. So while he was complaining of not seeing in the right eye, he was actually not seeing on the right side.
This is called a hemianopsia, which means ‘half no see’, or losing vision in one half of the visual field. Vision with hemianopsia is somewhat depicted in Figure 2. This is not an eye problem. This is a brain problem. Specifically, there is a problem in the left side of the occipital cortex, a part of the brain that gets signals from the eye.
Figure 2. Simulation of vision with right-sided hemianopsia. Everything to the right side of the visual field appears gray out or dark.
You see, our eyes ‘see’ things, but it’s really the brain that perceives the action of ‘seeing’ and gives meaning to it. When the brain suffers damage, both eyes will lose vision on the same side. But often patients will perceive the right side of vision loss as vision loss in the right eye.
And one of the most common causes of such brain damage is a stroke. Especially in a patient like John who has high blood pressure and heart problems. John had a history of congestive heart failure and had a pacemaker.
‘But I am not having a stroke. I feel fine.’ John said. I asked for several other symptoms, such as weakness or numbness on one side of the body, slurred speech, difficulty walking, and so on. He denied all of it.
He had been to the ED before, it was not a pleasant experience. He sometimes waited for 8 hours and just left before being seen.
I get that. But this time it is different. Hemianopsia can be the only symptom of a stroke. I managed to convince him to go that day. I also called his PCP to check up on him to manage his high blood pressure.
In the subsequent weeks, he developed other stroke symptoms including weakness in his leg.
I saw John again after 2 months. Needless to say, John was very distressed about his vision problem. He’s bumping into things and felt unsafe to drive. He complained about the long wait in the ED. The head CT scan did not reveal much, but he could not do the MRI due to his pacemaker. His visual field looked like in Figure 1C above. Well, not much improvement, perhaps a little worse even.
Research has shown that many stroke patients suffering hemianopsia recover partial or full vision within 6 weeks. He’s clearly not in the lucky team. If they don’t show any improvement by 6 months, it’s unlikely they will ever have improvement. About ⅓ of all stroke patients with hemianopsia will never recover or improve. I have seen some patients just like that, they permanently lose half of their visual field after a stroke.
I asked John to come back in 4 months, which will be 6 months post stroke, to check again.
This time his visual field looks like above (Figure 1D). It looked like he had a full recovery! I was relieved and felt very happy for him. I asked him, ‘how do you feel about your vision?’ I was surprised to hear him say, ‘Terrible. It’s getting worse.’
‘How come? Your visual field is much better. You are basically normal now.’
‘Oh THAT,’ he said, ‘yes that’s better, I can drive again. But my glasses are broken and I really cannot see anything for reading.’
You will be happy to learn that John now has new glasses and is seeing well. He’s seeing his PCP as well as his cardiologist to manage his high blood pressure.
No, the real character in this story does not look like this. Her eyes look identical from the outside.
I want to tell another story of pigment… in the back of the eye. A bit like the previous post, but no one has poor vision this time and it’s all happy… at least till now.
You know you can tell if a person is white or black or Asian or Hispanic usually by their appearance, right? A large part is the difference in skin color- no brainer here. But do you know that eye doctors can tell the racial differences by the color of the retina? Like the skin and iris (blue or brown eyed), the retina, the tissue in the back of the eye, is also lined by pigment cells that show different amounts of pigment. Similar to skin color, white people typically have less pigment in their retina, which shows up more pinkish in color compared to those of darker colors, eg, Asians. However, most of the time, the two eyes will be identical in coloration. So this lady’s eyes are really unique.
I first met her a few years ago, a healthy middle aged white female interested in new glasses and contact lenses. Her vision was normal and eyes healthy in every aspect, except when I looked at her retina with a lighted magnifier, I felt very confused. Her right and left retinas looked like they belonged to two different people- the right one being very light, just like from a typical white person, but her left retina looked much darker, as if she were Asian (Figure 1). I checked everywhere and both retinas looked completely healthy. There was absolutely nothing wrong with the retinas, just with different shades of pigment. This almost felt like a person had two arms or legs of different skin tones and that is not commonly seen unless a tanning session was done only on one side of the body.
Figure 1. Color photos of right and left eyes of the same person with a marked different hue. Copy right: Boston Eye Blink
Though everything looked normal, I did refer her to a retinal specialist.
She came back next year with a diagnosis of ocular melanocytoma in the left eye.
This is a condition that usually looks like this (Figure 2a) or this (Figure 2b). It’s typically a cluster of pigment cells forming a defined area of pigmentation that can be easily identified.
Figure 2. Examples of ocular melanocytoma. A) optic nerve melanocytoma. Copy right: New York Eye Cancer Center. B) Iris melatocytoma. Copy right: Ophthalmology and Visual Sciences, University of Iowa. In both images, an arrow points to the melanocytoma.
In my patient’s case, her pigment cells are diffused and dispersed, with almost no visible clumps, that it looks natural, smooth and just belongs. There is also no other pigment difference between the two eyes, including on eyelids, conjunctiva and iris. The secret only lies behind the eyes, unrevealed by a dilated retinal exam.
I think it’s marvelous that a pigment disorder turns out just right for her. It’s as beautiful as those people who have different eye colors, iris heterochromia (Figure 3), but it’s well hidden and more mysterious.
Figure 3. Iris heterochromia, where two eyes can be of different colors. Copy right: American Academy of Ophthalmology
It was the end of the clinic day. I finished my last patient’s chart and was ready to go, before noticing that a procedure result just popped out. I clicked into it, it’s a visual field testing result of a 60 year old gentleman I saw a few days ago. He complained that after ceiling plaster dropped into his right eye, his right eye could not see in the periphery.
This is a regular patient of mine. When the plaster incident happened 2 weeks ago I was on vacation so he saw another doctor in the practice. He initially went to the emergency room, received plenty of eye washing and antibiotic eye drops. He then saw my colleague two more times and according to the notes, his eye was recovering well. When I saw him his right eye was white and quiet, cornea completely healed, no defect, scar or edema. Internal structures of the eye were also normal. His visual acuity was 20/20. He did have trouble seeing fingers on the right side in his right eye. But his optic nerve appeared healthy. He’s a glaucoma suspect at baseline and I have been monitoring this over 2 years. The RNFL OCT that measures nerve thickness was stable to before. So the question is, why would he have a new visual field defect?
Dr. House says, patients always lie. He insisted that this problem came about after the plaster accident. ‘My eye is a mess’, he said. ‘First it hurt like hell for three whole days, then I cannot see out of my right eye’.
For a chemical injury to hurt the optic nerve, there had to be other signs, like inflammation in the anterior chamber, vitreous and retina. But there was none.
Also it made no sense that he’s losing vision from glaucoma progression, which is typically slow.
It happened suddenly so it’s not a tumor pressing onto his optic nerve either.
Could he be exaggerating because he was frustrated about the whole thing? After all, he waited in the ED for 4 hours, and he was on hold for scheduling to see eye doctors for a long time and did not get call backs.
Of course a formal visual field testing is in order. And that result just arrived in my inbox.
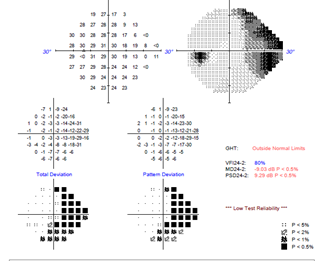
One peek at it, I knew I would not be going home any time soon (Figure 1).
Figure 1. Visual field testing result of the right eye (top image) and the left eye (bottom image). The dark color indicates that the patient was not able to see in that part of the visual field.
The right eye was not seeing the right side of things, just as he complained. Problem is, his left eye was also missing quite a few things on the right side. The left eye was much less severe and it was not picked up in the confrontational visual field test we did in the exam room.
This is what we call a hemianopsia (Figure 1), and it’s an emergency because a stroke was on the differential list.
I called him immediately. I advised him to go to ED immediately, even though he did not have any other stroke symptoms. He does have a history of heart attack and has a pacemaker.
I then called his primary care doctor and she was going to follow up with him.
Hemianopsia happens when one side of the brain that is in charge of vision becomes defective. This can happen with a stroke, a tumor or inflammation. In fact, according to the Cleveland Clinic, 70% of hemianopsia is due to stroke, 15% from brain tumors and 5% from bleeding in the brain [1]. Patients’ eyes can be completely normal, because the problem happens in the brain. It can happen as the only abnormal finding, without other telltale signs of a stroke. The dangerous part is that it is easily missed and over-looked, because the visual acuity can be 20/20, and you don’t find anything wrong with the eyes. Further, patients often describe this in a non-specific manner. Over the years I have heard ‘floaters in the left eye’, ‘my right eye is blurry’, or ‘my eye is a mess’. It is vitally important to always do a confrontational visual field and if suspicious, a formal visual field to clarify and confirm. Otherwise a critical, potentially life-threatening condition may be missed.
Hemianopsia from a stroke may improve over time though may not return to baseline completely, depending on the severity of the damage. Most start recovery within months of the stroke, but it may take up to 18 months for maximum recovery to occur [1]. I will see my patient in 3 months to check his visual field again. To help with vision deficit, certain prism may be used to expand the visual field, but that would the subject of another article.
Can your eye really pop out of your head? You see that in cartoons but can it happen to real people?
A group of our optometrist friends were chatting yesterday about this. One said that one of her patients told her about this history, and that she heard about this three times now from different sources. She did not see it herself but she was curious about it.
I remember such an incident of one of my patients. It was an African American lady in her 30s in good health. I was holding her upper eyelid up in order to examine the lower part of her retina, when she suddenly screamed and screamed, ‘Oh my god, my eye pops out!’ she screamed repeatedly. I almost panicked by her screaming. But I looked at her and saw that her eyelid was retracted and got stuck behind the eyeball and the eyeball was fine. So I gently massaged her upper lid and asked her to blink. A few seconds later her eyelid came down and all was normal. At this time, my technician who was working in the next room came knocking on the door and asked if everything was OK. I told her that all was good. My patient was a little embarrassed about her reaction and calmed down. The rest of the exam was uneventful and the patient left with an essentially normal eye exam.
Having that experience made me cautious about manipulating patients’ eyelids thereafter. Some people’s eyelids are loose and you can easily flip them. If they also happen to have protruding eyeballs, then the lids can get stuck behind the eyeball, which further limits the eyeball from moving.
I thought that eyeball popping out was a misnomer, it’s rather the eyelid going behind. If you think about it, the eyeball is secured by 6 external eye muscles to the eye socket, and the optic nerve which is like a cable also connects the eyeball to the brain. How can you easily get the eyeball out of the socket? If you could, I imagine there would be a lot of damage, potentially to the optic nerve and can cause vision loss. Sure with strong force such as in trauma, eyeballs can fly out of the socket, even the brain can burst out of the skull. But for a person to have spontaneous eyeball popping out, that would require a very high pressure behind the eye, and it just does not happen that easily.
However, it turns out that I did not know this subject well enough. It truely can happen in a condition called globe subluxation. Yes the eyelid could be stuck behind, but the eyeball is really out of (maybe partially) the eye socket. This can be caused by trauma, but it can also happen from triggers such as eyelid rubbing or straining badly.
Here is a photo from a real patient who suffered from globe subluxation. This is from a recent publication of a case report and all copyright belongs to the original authors and journal [1].
Figure 1. Spontaneous globe subluxation in a middle-aged woman [1]. Copyright in reference [1]
Quite a scene right? No doubt this is very unnerving to the patient as well as to the doctor!
According to this article, the most common risk factor associated with spontaneous globe luxation (SGL) is proptosis (that just means the eyeball is bulging) from having shallow orbits (eye sockets) or things growing in the back of the eyeball. The most common stuff growing behind the eyeball is actually from a condition called thyroid eye disease, in which excess fat and fibroblasts accumulate in the eye socket. Interestingly people with African descent tend to have shallow eye sockets and their eyes generally appear a little more bulging due to this reason. Other factors include loose tissues and muscles supporting the eye, loose eyelid, or having too much fat in the eye socket due to obesity.
So what harm does globe subluxation do? Seems obvious that an eyeball hanging out is an eyeball not working well for its function, which is seeing. Indeed, if this is severe or goes on for a long time, the optic nerve may be damaged, resulting in vision loss, sometimes permanent. On the other hand, when the eyeball is out, it’s not covered by the lids, and the surface drys out quickly, which can cause pain, light sensitivity and blurry vision immediately. If you think about it, our eyelids really do a good job protecting the eyeball, you can simply close your eyes. With eye protruding out like in the photo above, the eyeball is left there to dry up and exposed to the outside world should something hit or scratch on it.
So how do you pop the eyeball back in? First, relax. Then ask the patient to lay down with face up (or recline on your exam chair). Ask the patient to look down while you gently apply pressure on the globe downward and inward. You can use a cotton swab to roll the eyelids back while applying pressure to the globe [2].
Lastly, after the eye goes back to normal, we should probably do some investigation as to why it’s out in the first place. As mentioned above, thyroid eye disease, floppy eyelid syndrome, or maybe even a tumor behind the eye can make a patient prone to developing globe subluxation. So these need to be ruled out.
When I think back about my patient, I wonder if that’s actually not the first time this happened to her. She could not see her eyes, how would she know her eye popped out if she had no prior experience? To me, that was not a true globe subluxation, but rather an eyelid retraction. But her eyelid being so loose and retracting easily should also raise some suspicion on my part to work up further for thyroid eye disease and floppy eyelid syndrome.
According to literature, this is a very rare condition. However it can happen when maneuvering eyelids including when rubbing or inserting/removing contact lenses. I feel lucky that so far I have not encountered this with numerous patients that I have worked with for contact lens I/R training. But the moral of the story is that don’t touch your eyes, cause they can pop out (just exaggerating).
References
[1] Yadete, T., Isby, I., Patel, K. et al. Spontaneous globe subluxation: a case report and review of the literature. Int J Emerg Med 14, 74 (2021). https://doi.org/10.1186/s12245-021-00398-x